No one likes to think they or their loved ones might one day suffer from a debilitating illness. However, life threatening afflictions such as diabetes, cancer and heart disease are becoming all too common in western society.
Most people are understandably confused and frightened when they or someone they love are first diagnosed with a disease or disorder that may significantly affect quality of life and/or life expectancy. A large part of that fear comes from not fully understanding how or why it happened, and from the uncertainty of what’s going to happen next.
This section of the site provides an overview of some of the more common diseases and disorders plaguing the North American population today, including their known or suspected causes, consequences and ongoing disease management. A basic understanding of the disease process will help you know what questions to ask your doctor so that you can feel more empowered to take charge of your health. While you can’t change what’s happened, you can choose to manage your current situation in a positive, proactive manner in order to minimize any additional damage and maximize quality of life.
Please be advised this section provides brief overviews only (links to more detailed sources are provided for those interested in additional information), and the information should therefore in no way be considered complete; consult your health care professional for proper diagnosis and treatment.
Common Diseases and Disorders
(Click on each Disease/Disorder to reveal/hide details.)
|
 |
Definition: According to Wikipedia, arthritis (arthro – joint + itis – inflammation) is a general name that covers a large group of various different conditions involving damage to joints within the body. In fact, there are over 100 different diseases and conditions which affect the joints, the tissues surrounding the joints and other connective tissue.
Each disease or condition affects the joints a little differently, but general symptoms include pain and stiffness that can develop either gradually or all of a sudden. Some of these diseases/conditions involve the immune system and can even affect various internal organs.
The most common types of arthritis are listed below and more detailed information can be found in the specific write ups for them on this site:
- Osteoarthritis – a degenerative joint disease which can be related to trauma of the joint, infection of the joint or age.
- Gout – a common form of inflammatory arthritis where excess uric acid deposits in the joints cause mild to excruciating pain, redness, swelling and warmth.
- Fibromyalgia – chronic widespread pain with unusual sensitivity to what is generally non-painful stimuli.
- Rheumatoid arthritis – an autoimmune disease where the body’s immune system attacks the thin membrane lining the joints (synovium).
- Lupus – an autoimmune disease where the body’s immune system attacks the cell nucleus.
Known or suspected causes: Some forms of arthritis have specific known causes (i.e. gout) and specific infections can cause certain types of arthritis, but for many forms of arthritis the exact cause is still unknown.
Risk factors for arthritis include:
- Age – risk for most types of arthritis increases with age; however arthritis can strike at any age, including childhood.
- Gender – 60% of people with arthritis are women, however, gout is more common in men.
- Genetics – specific genes are associated with a higher risk of certain types of arthritis.
- Excess weight or obesity – particularly for osteoarthritis of the knee.
- Joint injuries – can lead to osteoarthritis.
- Infection – some types of infections can affect the joints and contribute to the development of some forms of arthritis.
- Occupation – repetitive knee bending and squatting can lead to osteoporosis of the knee.
Consequences of Arthritis: Arthritis is the most common cause of disability in the US, limiting activities of nearly 19 million adults.
Depending on the severity of the condition, one’s mobility and therefore one’s independence can be severely compromised. In many cases, the ability to grasp things firmly and/or perform tasks requiring fine motor skills is reduced or eliminated completely. Getting in and out of chairs, vehicles, bathtubs and sometimes even normal movements such as walking become extremely difficult and taxing on the body. Energy levels are therefore lowered so that people with arthritis find just getting through the day extremely exhausting.
The constant pain and frustration of not being able to do the things you want to do can lead to depression and the combined constant physical and mental stresses can then lead to other health issues.
Prevention/management: At this point in time there is no cure for arthritis, but early diagnosis and management can help decrease pain, slow the progression of the disease, improve function, and stay productive. This is especially important for inflammatory arthritis.
The main objective of treatment is to control pain, minimize joint damage and improve or maintain function and quality of life. Arthritis management strategies can help reduce pain and resulting physical limitations. The Arthritis Foundation Self Help Program and the Chronic Disease Self-Management Program are two effective self-management education programs.
It is important to remain physically active when you have arthritis despite the pain of doing so, because it has been shown that ongoing physical activity will decrease pain, improve function and delay disability. Low impact activities (i.e. walking, swimming, biking) and those which focus on improving range of motion (carefully moving the joint as far as it will go) are the most ideal.
Keeping a healthy body weight and protecting your joints will also slow the progression of the disease.
In more severe cases, physical or occupational therapy, splints or joint assistive aids and in some cases even surgery may be included as part of the treatment process.
Because the cause of many forms of arthritis is unknown, it is difficult to recommend prevention tactics. However, it has been shown that maintaining a healthy body weight and protecting joints will protect against osteoarthritis and that a healthy body weight will also reduce the risk of developing gout.
Additional information: The Arthritis Society of Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Foundation, Wikipedia

|
 |
Definition: Asthma is a chronic inflammatory disorder of the respiratory airways which obstructs air flow to the lungs. The obstruction is in most cases reversible either spontaneously (on its own) or with treatment.
Although a chronic obstructive condition, asthma is not classified as a chronic obstructive pulmonary disease (COPD) because asthma symptoms are generally reversible whereas COPD symptoms are not. However, left untreated asthma can create chronic inflammation in the lungs, leading to irreversible obstruction.
While asthma and allergies are related, they are not the same thing. An allergy is a (usually) harmless reaction to an inhaled, injected, swallowed or touched substance, whereas an asthmatic episode can be life threatening. Exposure to an allergen may cause irritation and swelling in specific areas of the body; allergens such as pollen, mould, animal dander and dust mites can make asthma worse by increasing sensitivity and inflammation in the airways.
Asthma symptoms are varied and recurring, and often include wheezing, coughing, tightness in the chest and shortness of breath. Symptoms can be mild, moderate or severe and can vary from person to person, as well as from one episode to the next. Asthma symptoms can flare up on occasion and then disappear for long periods.
As of yet there is no clear, measurable definition for asthma, and so a standard identification test is not yet available. Asthma is therefore currently diagnosed through evaluation of measurable symptoms. The disorder is classified based on 4 degrees of severity: intermittent, mild persistent, moderate persistent and severe persistent. Asthma can also be classified based on additional qualifying factors, as per the following examples:
- Status asthmaticus is acute asthma that does not respond to standard treatments of bronchodilators and steroids. It is life threatening and thus a medical emergency which can lead to cardiac or respiratory arrest.
- Brittle asthma is another type of asthma that does not respond to standard inhaled treatments. Brittle asthma is a rare condition which can be chronic (i.e. happens regularly) or acute (happens out of the blue).
- Exercise-induced asthma (E.I.A.) is shortness of breath induced by sustained aerobic exercise. Though it shares some similarities to regular asthma and even responds to some typical asthma medications, it does not appear to be caused by the same inflammatory reaction as regular asthma.
- Aspirin induced asthma is triggered by a hypersensitivity to aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs), and can cause an acute severe asthma attack within minutes or even hours of ingesting the NSAID. Symptoms can be quite severe, including violent broncospasm, shock, loss of consciousness and respiratory arrest. It is more common in cases of severe asthma, but up to 28% of adults with asthma (though rarely children) can be afflicted to some degree.
According to the Global Initiative for Asthma (GINA) Global Strategy for Asthma Management and Prevention Report (2009), the presence of asthma is increasing in most countries, particularly amongst children. The report estimates that asthma affects approximately 300 million people worldwide, and contributes to approximately 250,000 deaths per year. The lack of a precise and universally accepted definition for asthma makes it difficult to compare numbers reported from different parts of the world, but after standardizing some of the measurement methods GINA estimates the global presence of asthma ranges from 1% to 18% of the population in different countries. The analysis found asthma appears to be increasing in Africa, Latin America and parts of Asia, and decreasing in North America and Western Europe.
However, according to Wikipedia, asthma is a growing problem in the US – 9% of US children had asthma in 2001, compared to only 3.6% in 1980. African American and Latino children who live in cities are at the greatest risk for developing asthma. In some Latino neighbourhoods, as many as 1 in 3 children are living with the disorder. Wikipedia claims asthma affects 7% of the population of the United States and causes 4,000 deaths there per year.
The Asthma Society of Canada reports on their April 2005 fact sheet that while approximately 20 children and 500 adults die from asthma each year, 80% of these deaths could be prevented with proper asthma education. Although the Canadian death rate from asthma has slowly decreased since 1990, there were still on average 10 asthma-related deaths per week as of 2005.
Statistics Canada reports that as of 2009, 2,308,941 Canadians aged 12 and older are living with asthma, which represents 8.1% of the total Canadian population over the age of 12. 41% of these Canadian asthmatics are men (6.7% of the total male population over 12) and 59% are women (9.4% of the total female population over 12).
TripAtlas.com reports some studies have shown that asthma appears to be more prevalent in athletes than the general population. A survey of participants in the 1996 Summer Olympic games found that 15% had been diagnosed with asthma and that 10% were on asthma medication. However, it’s possible that athletes are simply diagnosed more often than the regular population, since even a mild form would interfere with performance and thus trigger an investigation into why. It’s also been suggested that some professional athletes may fake having asthma to get special permission to use certain performance enhancing drugs.
Known or suspected causes: It is generally accepted in medical circles that both environmental and genetic factors play a causal role in asthma. The Global Initiative for Asthma (GINA) differentiates between those factors which cause the development of asthma (primarily genetic) and those which trigger symptoms (typically environmental). However, they share a complex interrelationship that is still not fully understood. There is evidence to indicate that risk of asthma in a genetically susceptible person is affected by developmental aspects such as the maturation of the immune response (genetics) and the timing of infectious exposures during the first years of life (environment).
Asthma has a hereditary component, but there are multiple genes involved which may vary depending on ethnic background. In addition, a different set of genes determines how well a person will respond to various treatments.
GINA reports that sex is a risk factor for asthma. Male children under 14 are nearly twice as likely to have asthma as girls, but as they mature the risk drops so that by adulthood the prevalence of asthma is greater in women than in men. The reason for this has not been determined but it could have something to do with the fact that lungs are smaller in males than females at birth, but by adulthood male lungs have grown larger than female lungs.
GINA also reports that obesity is a risk factor for asthma, suggesting it’s possible that certain mediators such as leptin may affect airway function and therefore increase the likelihood of asthma developing.
Certain environmental factors have been linked to both the causation of asthma and the triggering of symptoms. There are over 300 known “occupational sensitizers” associated with occupational asthma (asthma caused by exposure to something in one’s work environment), and a comprehensive listing of occupational sensitizers can be found on the Massachusetts Labor and Workforce Development website (scroll to the bottom of the page). GINA estimates approximately 10% of adult asthma cases are triggered through occupational exposure, while a 2002 report by the American Thoracic Society indicates the number may be closer to 15%. Occupations associated with a high risk for occupational asthma include farming and agricultural work, painting (including spray painting), cleaning work and plastics manufacturing.
According to the World Health Organization, the strongest environmental risk factors for developing asthma are inhaled substances and particles that may provoke allergic reactions or irritate the airways.
The Asthma Society of Canada lists the following common asthma inflammatory triggers:
- Dust mites (the excretions and body parts of these tiny, spider-like creatures)
- Animals (dander, saliva, oil secretion, urine or feces)
- Cockroaches (feces)
- Moulds
- Pollens
- Viral infections
- Certain air pollutants
The site also lists several symptom triggers:
- Smoke
- Exercise
- Cold air
- Chemical fumes and other strong-smelling substances like perfumes
- Certain food additives like sulfites
- Certain air pollutants
- Intense emotions
Wikipedia identifies a number of suspected causal factors for asthma, as follows:
- Environmental tobacco smoke is associated with a higher risk of asthma and asthma morbidity (death due to asthma complications) in children.
- Outdoor air pollutants such as traffic pollution are also associated with an increased risk of childhood asthma.
- Viral infections are one of the most common triggers for asthma attacks, and lower respiratory tract (below the vocal chords) infections such as bronchiolitis may also increase one’s risk of developing asthma.
- Antibiotic use early in life has been linked to the development of asthma. It’s thought the antibiotics modify gut flora, which affects development of the immune system.
- The hygiene hypothesis suggests that a lack of early childhood exposure to infectious agents, symbiotic microorganisms (e.g., gut flora or probiotics), and parasites increases susceptibility to allergic diseases (such as asthma, hay fever and eczema) by suppressing natural development of the immune system. In other words, when a baby’s environment is too clean, its immune system is not challenged enough and so it doesn’t develop properly.
Consequences of Asthma: Asthmatic episodes vary in severity from person to person and from episode to episode. Episodes occur when airflow is obstructed while passing in and out of the lungs. Airflow can become obstructed when the lining of the airways becomes inflamed (irritated and swollen) and causes excessive mucous to be produced. In addition, when muscles surrounding the airways become sensitive they twitch and tighten, causing the airways to narrow further.
The airways of an asthmatic person are permanently inflamed to some degree, which makes them more sensitive to environmental triggers which exacerbate the inflammation and precipitate an asthma attack. Depending on the severity of the attack, symptoms can range from tightness in the chest, wheezing, shortness of breath and coughing to more serious and life threatening situations like shock, loss of consciousness, cardiac or respiratory arrest.
During asthmatic episodes, individuals may have difficulty talking and/or concentrating on what others are saying, due to lack of oxygen in the brain. This may also make them appear lethargic or confused. Their skin may take on a pale grey or bluish tint (cyanosis), particularly around the lips, eyes and nail beds, which indicates oxygen deprivation. Their wheezing and/or coughing will increase as their breathing becomes more shallow and either speeds up or slows down in response to the inability to take enough air into the lungs. The muscles on their neck may fire off while trying to help with the breathing process.
Asthma has the potential to severely affect one’s quality of life. Symptoms can interfere with sleep (asthmatic individuals may find their symptoms are worse in the evening and/or early morning, particularly when they lie down to sleep), work and recreational activities, causing people to take excessive sick days from work or school. In severe cases, emergency room visits and hospitalizations will not only play havoc with one’s schedule, they can also create excessive anxiety and stress for both the asthmatic individual and family members. Over time the narrowing of the airways will become permanent, thus making it harder to breathe even when asthma symptoms aren’t present, and side effects from long-term use of medications can lead to other physical problems.
According to the article Influence of comorbid conditions on asthma published in the European Respiratory journal, rhinosinusitis (rhinitis), gastro-oesophageal reflux disease (GERD), psychological disturbances, chronic infections and obstructive sleep apnea (OSA) are disorders often associated with asthma. The article claims:
- As many as 95% of asthmatics also suffer from rhinitis, suggesting that nasal and bronchial inflammation affect each other, possibly through a systemic effect.
- The majority of asthmatics suffer from GERD-like symptoms, possibly due to changes in pressure within the chest cavity or medications which affect the gastro-oesophageal sphincter. GERD, commonly known as acid reflux, can cause asthma symptoms, particularly coughing, when stomach acid travels up the esophagus and irritates the airways of the lungs.
- Obstructive sleep apnea (OSA) is commonly associated with asthma, perhaps due to increased airway collapsibility. This affects a person's ability to get a good night’s rest, which impacts on their overall general health and wellbeing.
- On average, asthmatics experience greater degrees of anxiety, depression and panic disorders than the general population.
According to an April 2009 article in Opthamology, asthmatic individuals who treat their asthma with inhaled and oral corticosteroids are at greater risk for developing cataracts. In addition, they are also at greater risk for developing corticosteroid induced osteoporosis.
Prevention/management: Because there is no known cure for asthma, treatment focuses on managing the disorder so that patients can live as normal and comfortably as possible. Individual triggers (such as cigarette smoke, pollution, pets or aspirin) need to be identified and avoided so that asthmatic episodes can be kept to a minimum.
Those on medication to help control their condition usually take two types:
- Controllers, or preventers, are taken daily to reduce inflammation in the airways so that over time patients experience fewer and fewer symptoms and therefore fewer and fewer asthma attacks. Controllers must be taken on a continuous basis or inflammation may return. Controllers do not immediately relieve wheezing, coughing or chest tightness and so should not be used to treat a severe asthma attack.
Glucocorticoids (a type of steroid) are the most effective long term treatment. They are usually inhaled, but if the asthma is severe then oral (ingested) steroids may also be required. Long acting beta-adrenoceptor agonists (LABD) are sometimes prescribed in addition to glucocorticoids since they have a 12 hour effect, but there is some controversy over their safety, particularly for children.
Because long-term glucocorticoid use is associated with increased risk of both cataracts and osteoporosis, ukotriene antagonists are sometimes prescribed as an alternative to inhaled glucocorticoids, but they are not as effective.
- Relievers are quick acting medications to alleviate symptoms during asthmatic episodes. They are a short term solution for an immediate problem, but do nothing to address inflammation. Side effects associated with relievers include increased heart rate, restlessness, tremor (shaky hands) and hyperactive behaviour in children, and so relievers should be used only as necessary. Excessive use (greater than 4 times per week) indicates the patient’s asthma is not well controlled.
The best types of relievers are short acting beta2-adrenoceptor agonists (SABA) such as albuterol. These relievers relax the smooth muscles around the bronchial tubes, which dilates the bronchial passages and facilitates oxygen flow. However, side effects such as insomnia, anxiety and tremor can occur.
A recent discovery by US researchers of a protein that might be linked to allergy-induced asthma could eventually lead to newer, more effective drugs to treat this disease.
Additional information: Asthma Society of Canada National Heart Blood and Lung Institute Centers for Disease Control and Prevention Mayo Clinic WebMD Wikipedia
|
 |
Definition: A painful, progressive condition caused by the compression of a key nerve (median nerve) at the wrist, resulting in pain, weakness, numbness and/or muscle damage to the wrist, hand or fingers.
The carpal tunnel is a narrow rigid passageway of ligament and bones at the base of the palm through which the median nerve passes to get to the hand. Swelling from irritated tendons or other sources can cause the passage way to narrow and the median nerve to compress. Symptoms usually start gradually, with burning, tingling or itching numbness in the palm and fingers, and the area may feel swollen even though there is no visual appearance of swelling. An electric-like shock feeling in the fingers or hand could also be experienced. Because many people sleep with flexed wrists, symptoms often first appear in the night. As the condition progresses, decreased grip strength may make it difficult to form a fist, and if untreated the muscles at the base of the thumb may waste away. The ability to distinguish between hot and cold may be lost.
Known or suspected causes: Carpal tunnel is generally caused by a combination of factors which increase pressure on the median nerve as opposed to something being wrong with the median nerve itself. It could be that those who succumb to this disorder are predisposed to it because they have a smaller than normal carpal tunnel.
Factors which can contribute to carpal tunnel syndrome include those which cause swelling to the wrist, such as sprain or fracture, repetitive strain injury, over activity of the pituitary gland, diabetes, hypothyroidism, rheumatoid arthritis, mechanical problems in the wrist joint, work stress, repeated use of vibrating hand tools, fluid retention during pregnancy or menopause, or the development of a cyst or tumor.
There is also some thought that a vitamin B6 (pyridoxine) deficiency can induce carpal tunnel syndrome.
According to the National Institute of Neurological Disorders and Stroke, while repetitive movement can cause bursitis or tendonitis, there is no clinical evidence to prove it causes carpal tunnel syndrome. However, CTS Central advises repeated grasping, turning and twisting can cause repetitive strain injury and this in turn can create swelling in the wrist area that puts pressure on the carpal tunnel.
The American Academy of Orthopaedic Surgeons claims carpal tunnel syndrome affects up to 10% of the population. They also claim that heredity is the most important factor.
Women are three times more likely to develop carpal tunnel syndrome than men, possibly because their carpal tunnels are generally smaller. Contraceptives can cause fluid retention, as can post menstrual syndrome (PMS). People with diabetes and other metabolic disorders which make nerves more susceptible to compression, as well as individuals who perform assembly line work (manufacturing, sewing, finishing, cleaning and meat/poultry/fish packing) are also at higher risk. Carpal tunnel syndrome is three times more common among assemblers than data-entry personnel.
Consequences Carpal Tunnel Syndrome: While the majority of patients recover fully, a full recovery can sometimes take months, and some people may need to change job duties or even jobs.
If the condition remains untreated, people may experience:
- Numbness or tingling in the palm of the hand and/or in the thumb and next two to three fingers;
- Pain in the wrist or hand which could extend to the elbow;
- Problems with fine finger movements – i.e. buttoning buttons;
- Wasting of the thumb muscles (in advanced cases) which may not be reversible;
- Weak grip – i.e. difficulty carrying bags, tendency to drop things, etc.;
- Loss of feeling in some fingers (in advanced cases).
Chronic pain can lead to depression and inability to use one’s hands as before can affect self esteem. In addition, a forced decision to switch careers or give up a rewarding hobby can be quite stressful.
Prevention/management: Prevention tactics include on-the-job conditioning, stretching exercises, frequent rest periods, correct posture and wrist position (avoid bending wrist all the way up or all the way down). Reduce force (i.e. hit cash register or computer keyboard keys more softly) and relax your grip (i.e. use a larger pen with a an oversized soft-grip adapter and free flowing ink so you don’t have to push so hard on the paper). Keep your hands warm and flexible (fingerless gloves can keep hands and wrists warm). Use properly designed equipment and tools to reduce risk of wrist injury.
To avoid permanent damage to the median nerve, early diagnosis and treatment are important. Initial treatment generally involves resting the hand/wrist for a couple of weeks, often bracing or splinting the area to avoid twisting or bending.
Non surgical treatments include drugs (nonsteroidal anti-inflammatory drugs, diuretics, corticosteroids), stretching and strengthening exercises (once symptoms have abated) or alternative therapies such as acupuncture or chiropractic care. Yoga has been shown to reduce pain and improve grip strength.
If symptoms persist for six months, surgery may be performed to cut the carpal ligament to enlarge the carpal tunnel. Physiotherapy is recommended after surgery to restore wrist strength.
Additional information: National Institute of Neurological Disorders and Stroke, Medline Plus, CTS Central, The American Academy of Orthopaedic Surgeons, MayoClinic.com
|
 |
Definition: Cancer can occur almost anywhere in the body, and is the result of a cell mutation which prevents cells from dying when they are supposed to. Thus cancerous cells continue to grow and multiply uncontrollably, eventually choking out healthy cells and compressing organs until the body can no longer function and death occurs. Some cancers remain localized, while others spread very quickly. As a general rule, the faster a cancer spreads, the worse the prognosis for survival.
According to the American National Cancer Institute, there are over 100 different types of cancer and most are named for the organ or type of cell in which they start. Non-melanoma skin cancer is the most common type of cancer among white people in the US, but because many of these skin cancers are treated in a doctor’s office it is difficult to estimate its true rate of frequency. After non-melanoma skin cancer, the following cancers are diagnosed most often in the US:
- Bladder cancer - Usually transitional cell carcinomas (see definition of carcinoma below) or TCC. Other types include squamous cell carcinoma and adenocarcinoma. According to the National Cancer Institute, squamous cell carcinoma and adenocarcinoma can develop in the inner lining of the bladder as a result of chronic irritation and inflammation.
- Breast cancer - Cancer that forms in breast tissue, usually in the duct tubes which carry milk to the nipple (ductal carcinoma) and the lobule glands which make milk (lobular carcinoma). Breast cancer can occur in both men and women, although it is much rarer in men.
- Colon and rectal cancer - Also collectively known as colorectal cancer or more commonly as bowel cancer, it includes cancerous growths in the colon, rectum and appendix. (Some definitions of colorectal cancer also include cancer of the anus.) According to Wikipedia, colorectal cancer is the third most commonly diagnosed cancer in the world, and is more common in more developed regions. Most colorectal cancers are adenocarcinomas. Colorectal cancers tend to start off as small mushroom shaped growths on the bowel wall called polyps or adenomas. These growths may also be classified as adenomatous polyps.
- Endometrial Cancer - Cancer that forms in the endometrium (or inner lining) of the uterus. There are several different types of endometrial cancers, with the most common being endometrioid adenocarcinoma. Endometrial carcinomas can be classified as Type I (low grade, less aggressive) or Type II (high grade, more aggressive high grade carcinomas such as uterine papillary serous carcinoma and uterine clear cell carcinoma). Endometrial stromal sarcomas, which occur in the non-glandular connective tissues, are less common than the carcinomas. In rare instances, these two cancer types (carcinoma and sarcoma) can both be present.
- Kidney (Renal Cell) Cancer - Renal cell carcinoma (RCC) is cancer of the proximal tubules. RCC is the most common type of kidney cancer, responsible for approximately 80% of all kidney cancers in adults. It is one of the most lethal cancers, resistant to both radiation therapy and chemotherapy. The second most common type of kidney cancer, transitional cell carcinoma or TCC (see bladder cancer info above) occurs in the renal pelvis. There are also other less common forms of kidney cancer, including Wilms' tumor, a type of kidney cancer that most often occurs in children under the age of 5.
- Leukemia - Cancer that forms in the bone marrow and causes too many blood cells to be produced. Leukemia can either be acute or chronic. It can also be classified as lymphoblastic/lymphocytic leukemia or myeloid/myelogenous leukemia. Lymphocystic and myelogenous leukemias can be classified as either chronic or acute. There are a few additional types of leukemia (most are relatively rare), including adult T-cell leukemia, which is caused by the human T-lymphotropic virus (HTLV) which "immortalizes" T-cells so that they are able to proliferate abnormally.
- Lung Cancer - Cancer that forms in lung tissue, usually in the epithelial cells lining air passages. The two main types are small-cell lung carcinoma and non-small cell carcinoma. The lungs are a common place for secondary cancers to develop. Cancers which start in the lungs (primary lung cancer) most often metastasize (travel) to the adrenal glands (glands which sit on top of the kidneys and secrete hormones into the blood), liver, brain and bone.
- Melanoma - Cancer that starts in melanocytes, which are cells that produce melanin (pigment). Most melanocytes are found in the bottom layer of the epidermis (outermost layer of the skin) and in hair, and are primarily responsible for skin and hair colour. Melanocytes can also be found in the middle layer (uvea) of the eye, the inner ear, meninges (membranes which envelope the central nervous system), bones and heart. Melanoma is less common than other skin cancers, but more deadly. Once it reaches the blood vessels lower down in the skin, it can spread throughout the body via blood or lymph vessels. While melanoma is generally classified as skin cancer, it can also start in the other melanocytes-containing tissues noted above.
- Non-Hodgkin Lymphoma (NHL) - A diverse group of blood cancers (other than Hodgkin Lymphoma) involving lymphocytes (white blood cells). There are a number of types of NHL, some aggressive (fast-growing) and some indolent (slow growing). Some involve B-cells and some T cells.
- Pancreatic Cancer - Cancer of the pancreas, which is a gland situated in the digestive tract (stomach/intestines) area of the body. Pancreatic cancer is one of the deadlier cancers, perhaps in part because there are usually no symptoms until the disease is fairly advanced. About 95% of pancreatic cancer is adenocarcinoma.
- Prostate Cancer - Cancer that forms in the male prostate gland. Most cancers of the prostate are adenocarcinomas. They tend to develop in older men, with the average age of diagnoses being 70 (as per Wikipedia). Prostate cancer usually grows very slowly (only a small percentage of prostate cancers are the more aggressive small-cell carcinoma or squamous cell carcinoma), so that many men who are diagnosed with prostate cancer will evenutally die of other natural causes.
- Thyroid Cancer - Cancer that forms in the thyroid gland. There are 4 main types of thyroid cancer, all of them carcinomas: papillary thyroid cancer, follicular thyroid cancer, medullary thyroid cancer and anaplastic thyroid cancer. Other possible types include lymphoma, squamous cell carcinoma and sarcoma. Most thyroid cancers occur in women,
In addition to location, cancers are also classified by the type of cell tissue affected. The National Cancer Institute defines the main cancer types as follows:
- Carcinoma - cancer that begins in the epithelial cells of the outer skin and tissues that line or cover internal organs. There are different types of carcinoma, depending on where the cancer is located. For example, adenocarcinoma occurs in glandular tissue, squamous cell carcinoma develops in squamous epithelial cells and basal cell carcinoma grows in the deepest layer (basal layer) of the skin.
- Sarcoma - cancer that begins in bone, cartilage, fat, muscle, blood vessels, or other connective or supportive tissue. Like carcinomas, sarcomas can be further classified according to their source - osteoscarcoma occurs in bone tissue, chondrosarcoma develops in cartilage and leiomyosarcoma grows in smooth muscle.
- Leukemia - cancer that starts in blood-forming tissue such as the bone marrow and causes large numbers of abnormal blood cells to be produced and released into the blood. Leukemia can either be acute or chronic. It can also be classified as lymphoblastic/lymphocytic leukemia or myeloid/myelogenous leukemia. Lymphocystic and myelogenous leukemias can be classified as either chronic or acute. There are a few additional types of leukemia (most are relatively rare), including adult T-cell leukemia, which is caused by the human T-lymphotropic virus (HTLV) which "immortalizes" T-cells so that they are able to proliferate abnormally.
- Lymphoma and myeloma - cancers that begin in the cells of the immune system. Lymphoma cancers often originate in lymph nodes, but can also affect other organs including the skin, brain, bowels and bone. Myeloma is cancer of plasma cells, which are a type of white blood cell that produces antibodies to fight foreign invaders (i.e viruses, bacteria, mould). Cancerous plasma cells accumulate in the bones and bone marrow, causing bone lesions and interfering with the production of normal blood cells.
- Central nervous system cancers - cancers that begin in the tissues of the brain and spinal cord. There are a number of different types of brain tumours, such as glioma, oligodendroglioma, ependymoma, meningioma, lymphoma and schwannoma. Breast and lung cancers are the cancers which most often metastasize (spread from other parts of the body) to the brain.
Cancers can be classified by their degree of growth. As a general rule (there are a number of exceptions), Stage I refers to a small localized growth that hasn’t yet metastasized (spread) elsewhere in the body. Stage II refers to a larger growth that is still localized. Stage III means the cancer has spread to tissue or lymph nodes adjacent to the original growth. Stage IV means the cancer has spread to other parts of the body.
Finally, cancers can also be classified by their degree of differentiation from normal cells. Well-differentiated means the cancer cells look very much like normal cells under a microscope and share some similar functions. Because of this, well-differentiated cells tend to respond well to anti-cancer drugs or radiation therapy. On the other hand, undifferentiated or poorly-differentiated cells are more primitive than normal cells, act autonomously and rarely respond to drug or radiation treatment. Grade 1 cancers are well differentiated, grade 2 are moderately well differentiated and grade 3 are poorly differentiated cancer cells. Thus the higher the grade, the worse the prognosis.
Cancer cells can spread to other parts of the body through the blood and lymph nodes. The site where the cancer originally begins is called the originating or primary location and the site where the cancer travels to is called the metastasized or secondary location. For example, cancer may start in the breast (originating/primary site) and travel to the brain (metastasized/secondary site). In this example, lab analysis of the cancerous tissue in the brain would show the cancer to be composed of breast cells, indicating the cancer originally started in the breast. Cancer for which a primary site cannot be found is called cancer of unknown primary.
Known or suspected causes: While scientists do not fully understand cancer, our knowledge is growing. We now know that in order for a malignant tumour (i.e. cancer) to develop, two things need to happen. First, normal cells have to mutate into cancer cells. Second, these cancerous cells require a blood supply in order to grow.
A large number of possible contributors (or risk factors) to cell mutation have been identified; I will discuss a number of them below. (Please be aware this is no means an exhaustive list, but it does include some of the major risk factors you should be aware of. Most of this information has been taken from the National Cancer Institute web site, and you can visit this site to learn more about the known risk factors for a wide variety of cancers.) The process by which a malignant tumour obtains access to a blood supply is called angiogenesis, which controls the growth of blood vessels. (See my article Can We Eat to Starve Cancer for further information on this very interesting subject. While the theory behind eating certain foods to prevent cancer has not yet been proven in the lab, it is the subject of considerable attention and research.)
There is a genetic component to many cancers, in that your odds of developing certain cancers are higher if other family members have already had the same type of cancer. Genetics is, unfortunately, beyond our control, as is age, which increases the odds of developing certain cancers such as breast, colorectal, non-Hodgkin lymphoma, prostate and thyroid cancer.
However, there are many risk factors for cancer well within our control, such as smoking and obesity. Of the 12 types of cancers outlined above, smoking has been linked to 6 of them - lung, bladder, colorectal, kidney, acute myeloid leukemia and pancreatic cancer. Other cancers linked to smoking include esophagus, larynx (voice box), mouth, throat, stomach and cervix.
The National Cancer Institute reports risk for the following cancers may be increased as much as 30% in obese and sedentary individuals: colon, breast (postmenopausal), endometrium (the lining of the uterus), kidney, and esophagus. There is also some evidence to indicate that obesity plays a factor in the development of gallbladder, ovary and pancreatic cancer. Although the connection is not fully understood, one theory suspects that alterations in sex hormones (e.g., estrogen, progesterone, and androgens), insulin and IGF-1 play a key role. Another possible explanation is that excessive eating (as well as eating poorly) increases the body’s exposure to free radicals, damaging cells so that they mutate and become cancerous.
Chemical exposure can increase one’s risk of certain cancers. For example:
- Risk of bladder cancer is increased for individuals in the dye, rubber, chemical, metal, textile and leather industries. Hairdressers, machinists, printers, painters and truck drivers are also at risk.
- Arsenic exposure has been linked with increased odds of developing bladder cancer, as well as basal cell and sqamous cell skin cancers. Arsenic is a poisonous metal which occurs naturally in nature and can sometimes contaminate drinking water. Arsenic is used as a strengthening agent for metals such as copper and lead and is also used extensively in electronic equipment as a semi-conductor.
- Exposure to benzene, widely used in the chemical industry and also found in cigarette smoke and gasoline, is a risk factor for leukemia. Benzene is used in the production of plastics, resins, nylon and other synthetic fibers, rubbers, lubricants, dyes, detergents, drugs, and pesticides.
- Exposure to asbestos, arsenic, chromium, nickel, soot, tar, radon and other substances can lead to lung cancer. Risk increases proportionately with length of exposure.
- Air pollution has been associated with a slight risk of lung cancer.
- Radiation exposure (diagnostic x-rays, radioactive fallout from incidents such as Chernobyl and the Japan Tsunami) can increase the risk of thyroid cancer.
Some treatments for one type of cancer can increase the risk of developing an alternate type of cancer.
- Certain cancer drugs such as cyclophosphamide have been linked with bladder cancer. Cyclophosphamide is a chemotherapy drug that works by slowing or stopping cell growth.
- Tamoxifen, a drug used to prevent or treat breast cancer, can increase risk of uterine cancer. Certain cancers require the female hormone estrogen in order to grow. Tamoxifen binds to estrogen and thus prevents the cancer cells from being able to use it.
- Radiation therapy, particularly if received under the age of 30, is associated with increased risk of breast cancer (with radiation to the chest area) and uterine cancer (with radiation to the pelvis). It has also been associated with basal cell and squamous cell skin cancers.
- Certain chemotherapy drugs have been linked with a small risk of developing acute leukemia.
UV radiation is the greatest risk factor for any type of skin cancer.
- Lifetime sun exposure affects level of risk.
- Artificial UV via sunlamps and tanning booths, particularly before age 30, also affect skin cancer risk.
Additional risk factors for breast cancer include:
- Having more dense (as opposed to fatty) breast tissue.
- Never having children.
- Having your first child at a later stage in life.
- Having your first period prior to age 12.
- Going through menopause after age 55.
- Taking menopausal hormone therapy for an extended period.
- Being white as opposed to African American/black, Hispanic/Latina, Asian/Pacific Islander or American Indian/Alaskan Native.
- Lack of physical activity.
- Drinking alcohol.
Additional risk factors for colorectal cancer include:
Additional risk factors for endometrial cancer include:
- Endometrial hyperplasia (abnormal overgrowth of endometrium, the inner lining of the uterus).
- Never having children.
- Having your first period prior to age 12.
- Going through menopause after age 55.
- Taking estrogen on its own as menopausal hormone therapy for an extended period.
Additional risk factors for melanoma include:
- A large number of “common” moles, which are generally smaller than a pea, have an even colour (pink, tan or brown), and are round or oval with a smooth surface.
- A dysplastic nevus mole, which is usually larger than a common mole and is generally flat with a smooth, slightly scaly or pebbly surface and irregular edges.
Additional risk factors for Non-Hodgkin Lymphoma include:
Additional risk factors for pancreatic cancer include:
Diabetes.
Chronic pancreatitis.
Consequences of Cancer: Depends on the type of cancer as well as the degree of progression prior to detection. Left untreated, most cancers are fatal. Because there are so many different types of cancer, and the fact that each type of cancer can mainfest differently from person to person, there is no one treatment plan which will work for everyone. However, as a general rule, treatment may include surgery for removal of affected area, radiation treatment, chemotherapy, or a combination of the three.
Radiation is painless and side effects are usually temporary and vary depending on the location of the body undergoing treatment. Chemotherapy taxes the immune system, so when undergoing this type of treatment one needs to eat well to keep the immune system strong and avoid contact with people who have a cold or the flu.
Prevention/management: While there are no guarantees in life, the best way to prevent cancer is to live as healthy a lifestyle as possible, so that your immune system remains strong and your exposure to risk factors is minimized. This means keeping your weight under control, eating a healthy diet that is low in fat and high in fruits and vegetables, and staying active as much as possible.
In addition, it would be prudent to avoid smoking and second hand smoke, excessive exposure to sunlight and heavy drinking. You may wish to use more natural cleansers when cleaning your home and doing laundry, and use perfume and other scented products sparingly.
Cancer screenings, such as mammography and breast examination for breast cancer and colonoscopy for colon cancer, may help catch cancer at the early, most treatable stages. Some people at high risk for developing certain cancers can take medication to reduce their risk, although there could be long term side effects associated with the medication.
Additional information: National Cancer Institute Canadian Cancer Society Oncolink American Cancer Society ProstateCancerGuide.net Wikipedia
|
 |
Definition: Celiac disease is an autoimmune disease of the small intestine, caused by an abnormal immune reaction to gluten. Consumption of gluten causes the body’s immune system to produce an inflammatory response which damages or destroys the villi of the small intestine, which in turn interferes with the proper absorption of nutrients. While the disease is caused by a reaction to wheat proteins, it is not the same as wheat allergy. Allergies are conditions that people can sometimes grow out of, but this is not the case with celiac disease.
A review of the available literature commissioned by the Food Allergy Task Force of the European branch of the International Life Sciences Institute (ILSI Europe) suggests that celiac disease is genetically determined (i.e. inherited) and more common in women than men.
Once considered a rare childhood disease, greater awareness and testing have increased diagnosis rates and it is now recognized that celiac disease is much more widespread than previously thought. Exact numbers vary, but the National Institutes of Health (NIH) estimates up to 1 percent of all Americans suffer from celiac disease, though many have not been properly diagnosed. A 2003 study, Prevalence of Celiac Disease in At-Risk and Not-At-Risk Groups in the United States, determined that on average 1 in every 133 people in the US has celiac disease, and that first degree relatives of celiac disease patients have a 1 in 22 chance of being diagnosed with it as well. The Canadian Celiac Association similarly estimates that 1 in 133 Canadians have the disease.
People with celiac disease tend to have other autoimmune diseases such as type 1 diabetes, autoimmune thyroid disease, autoimmune liver disease, rheumatoid arthritis, Addison’s disease (glands which produce critical hormones are damaged) and Sjцgren’s syndrome (glands which produce tears and saliva are destroyed). This has lead scientists to speculate that the connection between celiac disease and these other autoimmune diseases may be genetic.
Known or suspected causes: While celiac disease is not well understood, it is generally accepted there is a genetic factor present and that the genes involved are related to immune system function. However, a trigger is also required before the disease becomes active.
There are several theories as to what these triggers might be, with infection by either the rotavirus or the human intestinal adenovirus being two prominent possibilities.
A 2005 observational study found that babies with increased risk for celiac disease exposed to wheat, barley or rye within the first three months after birth were five times more likely to develop celiac disease when compared against increased risk infants who were not exposed until 4-6 months of age. One possible explanation is that the baby’s intestinal flora (microorganisms that live in the digestive tract) have not yet fully developed; one of the first types of intestinal flora to colonize the digestive tract are microorganisms which help to develop our immune system.
Another study suggests that prolonging breast feeding up to the point at which gluten is introduced into the diet may have a protective effect against celiac disease. However, there is no evidence to indicate whether breastfeeding provides permanent protection or simply delays the onset of symptoms.
Although often diagnosed in childhood, celiac disease can manifest at any age and is sometimes triggered after surgery, pregnancy, childbirth, viral infection, or severe emotional stress.
Consequences of Celiac Disease: The consequences of celiac disease can be quite severe. As more and more intestinal villi are destroyed, less and less nutrients can be absorbed by the body, leading to malnutrition, osteoporosis, anaemia and other vitamin and mineral deficiencies, as well as other more life threatening conditions such as liver disease, possibility of hemmorrhage and significantly increased risk of intestinal cancer. Additional complications include hyposplenism, gall bladder malfunction, pancreatic insufficiency, ulcerative jejunitis, stricturing, central and peripheral nervous system disorders and other neurological manifestations (caused by nutrient deficiencies).
One of the reasons why celiac disease can go undetected for quite some time is that symptoms vary from person to person, and digestive symptoms can be incorrectly diagnosed as irritable bowel syndrome. Problems may manifest not only in the digestive tract, but also in other parts of the body. A person with celiac disease may not even have detectible symptoms, but damage to the small bowel can occur even when no symptoms are present.
Digestive symptoms are more common in infants and young children and may include abdominal pain, bloating and distension, chronic diarrhea, vomiting, constipation, pale, malodourous or greasy stool (steatorrhoea), weight loss or failure to gain weight and general irritability. Malabsorption of nutrients can cause failure to thrive in infants, as well as delayed growth and short stature, delayed puberty, and dental enamel defects of the permanent teeth.
Adults, on the other hand, are less likely to have digestive symptoms, and more likely to exhibit one or more of the following: unexplained iron-deficiency anaemia, fatigue and/or weakness with lack of energy, bone or joint pain, arthritis, bone loss or osteoporosis, depression or anxiety, tingling numbness in the hands and feet, migraines, central and peripheral nervous system disorders and other neurological manifestations, seizures, missed menstrual periods, infertility (both male and female) or recurrent miscarriage, canker sores inside the mouth and/or dermatitis herpetiformis.
Prevention/management: There is no known “cure” for celiac disease, and currently the only effective treatment is following a strict gluten-free diet. Doing so permits the intestines to heal, which usually resolves all symptoms and, depending on how soon the diet is started, can also reduce the heightened risk for osteoporosis, cancer and other potential complications.
A small percentage of celiac disease patients suffer from refractory disease, meaning they do not improve on a gluten-free diet. This could be because the intestinal damage was so great the intestines are not able to heal on their own, or because the patient is not adhering to a gluten-free diet, either deliberately or accidentally. Unfortunately, the term gluten-free is not regulated the same way in all countries, and more often than not “gluten-free” is used to describe a food product containing minimal amounts of gluten as opposed to zero gluten content. If dietary consumption has been ruled out, steroids or immunosuppressants might be prescribed.
As noted above, there is some evidence to indicate that delaying exposure to gluten in newborns until the age of 4 months may reduce the risk of these babies developing celiac disease if they are genetically predisposed to it. Breastfeeding up until the time of first exposure may also provide some protective benefits.
Because celiac disease is associated with several other medical conditions, patients should be monitored periodically for complications such as iron, folic acid and vitamin B12 deficiencies, hypocalcaemia (low calcium levels), hypothyroidism (underactive thyroid) and osteoporosis (loss of bone mineral density).
Additional information: Celiac Disease Foundation Canadian Celiac Association National Digestive Diseases Information Clearinghouse (NDDIC) Celiac.com Wikipedia
|
 |
Definition: Profound fatigue not improved by bed rest and which may be worsened by physical or mental activity, causing a person to operate at a much lower activity level with much less stamina than before. There are eight other characteristic symptoms: post exertional malaise (relapse of symptoms after physical or mental exertion); unrefreshing sleep; substantial impairment in memory/concentration; muscle pain; pain in multiple joints; headaches of a new type, pattern or severity; sore throat and tender neck or armpit lymph nodes.
Other symptoms which may occur include weakness, insomnia, abdominal pain, alcohol intolerance, bloating, irritable bowel, allergies or sensitivities to foods, odors, chemicals, medications or noise, chest pain, chronic cough, diarrhea, dizziness, balance problems or fainting, dry eyes or mouth, visual disturbances (blurring, sensitivity to light, eye pain), earaches, irregular heartbeat, jaw pain, morning stiffness, nausea, poor temperature control, intolerance to heat and cold extremes, night sweats, psychological problems (depression, irritability, mood swings, anxiety, panic attacks), shortness of breath, skin sensations, tingling sensations, seizures and weight loss.
The majority of cases start suddenly and are usually accompanied by a flu-like illness or respiratory infection (like bronchitis) that never really resolves and eventually evolves into CFS. Quite often this occurs in the winter, although sometimes it can be within a few months of severe adverse stress. Other cases have a much more gradual onset, sometimes spanning multiple years.
To be clinically diagnosed, a patient must have severe chronic fatigue for at least six months (with other known medical conditions excluded by clinical diagnosis) and concurrently have four or more of the following symptoms for a similar period of time and which weren’t already present prior to the onset of the fatigue: substantial impairment in short-term memory or concentration; sore throat; tender lymph nodes; muscle pain; multi-joint pain without swelling or redness; headaches of a new type, pattern or severity; unrefreshing sleep; and post-exertional malaise lasting more than 24 hours.
Known or suspected causes: At this time there are no known causes of CFS and no specific diagnostic tests are available. A significant amount of research has been dedicated to discovering the underlying cause of CFS, but to date no definitive answers have been found. Researchers are currently exploring several possibilities, including environmental and genetic factors, a possible viral connection, and the role of the immune, endocrine and nervous systems in the development of CFS.
Since incapacitating fatigue is a symptom of many illnesses, other known conditions (such as sleep apnea, lyme disease, thyroid conditions, diabetes, multiple sclerosis, COPD, various cancers, depression and bipolar disorders) must be ruled out before a diagnosis of CFS can be made.
CFS can affect people of every age, gender, ethnicity and socio-economic group, although women are afflicted four times as often as men. (However, this could be simply that women are more likely than men to report their symptoms to a doctor.) The disorder appears to be most common in people in their forties and fifties, and although it is less common in children than adults, children can develop CFS, particularly during the teen years.
CFS is occasionally seen in members of the same family, and although more research is required, current thinking is that there may be a genetic link as opposed to the disorder being contagious.
Consequences of Chronic Fatigue Syndrome: FM-CFS Canada estimates anywhere from 1-1.5 million Canadians suffer from either CFS or fibromyalgia (the organization combines the statistics from the two diseases, likely because many of their symptoms are similar) and that total annual cost associated with these diseases exceeds $3.48 billion. There has never been a detailed study done on the prevalence of CFS in Canada, but based on the limited estimates of the 1999 DePaul University Prevalence Study (Chicago), CFS is twice as prevalent as multiple sclerosis (MS) and five times more common than AIDS.
Because CFS is difficult to diagnose, the US Center for Disease Control and Prevention (CDC) estimates that 80% of CFS sufferers have not been diagnosed. The earlier a person receives medical treatment, the greater the likelihood the illness will resolve, but only about half the people with CFS have consulted a doctor. CDC research indicates that those people diagnosed with the disease within two years were more likely to improve through treatment than those who remained undiagnosed and untreated for longer than two years.
Between 1 and 4 million Americans suffer from CFS and at least a quarter of them are unemployed or on disability due to it. The extreme fatigue causes a substantial reduction in daily activities, and can prove as disabling as multiple sclerosis, lupus, rheumatoid arthritis, congestive heart failure and similar chronic conditions. A reduced activity level may lead to deconditioning so that one is more prone to other conditions such as muscle weakness, obesity and all the issues that go along with it such as high blood pressure, diabetes and heart disease, etc.
Severity of symptoms will vary from person to person so that some people will remain homebound while others improve enough to resume working and other personal/social activities despite still experiencing ongoing symptoms. Only about 5-10% of people will make a full recovery.
When symptoms are particularly severe, depression, social isolation caused by fatigue, lifestyle restrictions and a loss of independence, livelihood and economic security can be extremely stressful on both the individual and their families. Because there are no outward signs of CFS, skepticism and misconceptions about the illness can make it difficult for family members to understand and cope with the daily limitations and future uncertainties associated with the disease. Individual and/or family education and counseling may prove helpful in many cases.
Prevention/management: There is no known cure for CFS and so treatment is aimed at relieving symptoms and improving function. A combination of drug (for sleep, pain and other specific symptoms) and non-drug therapies (lifestyle changes and carefully supervised physical activity) are usually undertaken, but no single therapy will help all CFS patients equally.
Lifestyle changes include pre-planning activities to be done during that part of the day when you have the most energy, making lists and reminder notes to offset tendencies for forgetfulness, getting enough sleep, pacing yourself to prevent over exertion, stress reduction, dietary restrictions, nutritional supplementation and gentle stretching. Exercise can be helpful, although care must be taken not to overexert and consequently exacerbate symptoms.
Quite often symptoms are cyclical in that they swing from being severe to quite mild and at times into a full temporary remission. It is important not to overdo things during these periods of remission when a person is feeling better as this can cause a relapse.
Additional information: There is some concern that the name chronic fatigue syndrome trivializes the disease and several advocacy groups would like to see the name changed. The World Health Organization uses the term post viral fatigue syndrome and another alternative name for CFS being promoted is chronic fatigue immune dysfunction syndrome.
FM-CFS Canada, Centers for Disease Control and Prevention, Wikipedia, Medline Plus, FamilyDoctor, Mayo Clinic, CFIDS Association of America
|
 |
Definition: Congestive heart failure occurs when the heart is no longer capable of supplying enough blood to meet the needs of the body. When the kidneys do not receive an adequate blood supply, they are unable to adequately filter fluid from the circulatory system and release it as urine. The resulting fluid build-up in the body is called “congestion”, which is why this condition is called “congestive” heart failure.
Congestive heart failure can result from a variety of causes, as outlined below. It is classified as a chronic condition, which means it occurs slowly over time, and it can often be treated with lifestyle changes and/or medication to slow the progression of the disease. However, congestive heart failure can be suddenly worsened by events such as heart attack, pneumonia, uncontrolled hypertension (high blood pressure), straying from a diet which controls fluid build-up, taking medications (i.e. NSAIDS, certain steroids, or thiazolidinediones) which increase fluid build-up, etc. This may lead to
acute decompensated heart failure, which creates a respiratory distress situation and thus requires immediate medical attention.
There are two ways the medical community classifies heart failure – how it affects you functionally in your day to day tasks and what stage of the disease your body is physically at.
The New York Heart Association Functional Classification is the generally accepted standard, which divides congestive heart failure into 4 classes, as follows:
- Class I – no symptoms or limitations experienced during ordinary activities
- Class II – slight or mild limitation of activity, but the person is still comfortable at rest or with mild exertion
- Class III – marked limitation of any activity in that the person is only comfortable when at rest
- Class IV – any physical activity will bring on discomfort and symptoms occur even at rest
The American College of Cardiology/American Heart Association working group has defined the various physical states of the disease as follows:
- Stage A – a person is at high risk for developing congestive heart failure in the future (refer to known or suspected causes section below) but there is currently no functional or structural heart disorder
- Stage B – a structural disorder exists but no symptoms are experienced
- Stage C – symptoms of heart failure exist, but can be managed by medical treatment
- Stage D – the disease is advanced enough that hospital-based support, heart transplant or palliative care is required
According to a 2005 study reported in The Lancet approximately 2% of adults in developed countries suffer from heart failure, but the prevalence increases to 6-10% for the over 65 age group. eMedicineHealth claims that heart failure affects 1% of people over 50 years of age, 5% of people over 75 and 25% of people over 85. The site also notes that close to 5 million peole in the US have congestive heart failure, there are about 550,000 new cases each year and the condition is more common among African Americans than whites.
Known or suspected causes: There are many known causes of congestive heart failure, including diseases which either weaken or stiffen the heart muscle so that it is no longer able to pump blood as efficiently, physical conditions which dramatically increase the body’s need for oxygen, and structural defects within the heart itself.
Diseases which can damage the heart muscle include myocardial infarction (heart attack) and other forms of ischemic heart disease, hypertension (high blood pressure), valvular heart disease, hemochromatosis, amyloidosis and other forms of cardiomyopathy.
The following conditions can increase the body’s need for oxygen to a point where the heart is unable to meet these additional demands: anemia, gram negative septicaemia, Beriberi, thyrotoxicosis, arteriovenous fistulae or other arteriovenous malformations. This particular type of heart failure is known as “high output” heart failure.
Structural heart defects can interfere with the heart’s pumping ability. Leaky valves can interrupt the normal flow of blood, rendering the heart muscle less efficient. These heart defects can be present at birth, or they could develop later on in life.
In 2001, the National Health and Nutrition Examination Survey released a 19 year study of 13,643 healthy adult men and women which reported that incidences of congestive heart failure were on the rise in the US. Through examination of medical records and death certificates, the authors of the study identified the causes of the 1382 congestive heart failure incidents which subsequently developed in these 13,000+ adults and identified the following population attributable risk (PAR) factors:
| | PAR |
| Coronary heart disease | 61.6% |
| Cigarette smoking* | 17.1% |
| Hypertension | 10.1% |
| Low physical activity* | 9.2% |
| Male sex | 8.9% |
| High school education only | 8.9% |
| Being overweight | 8.0% |
| Diabetes | 3.1% |
| Valvular heart disease | 2.2% |
*For women only, the PAR risk factors for cigarette smoking and physical inactivity increased to 21.5% and 13.2% respectively.
In addition to the above risk factors, studies have shown the following have also been associated with congestive heart failure:
- Abuse of drugs such as alcohol or cocaine
- Use of certain pharmaceutical drugs such as chemotherapeutic agents (to fight cancer)
- Having obstructive sleep apea, which blocks airways and thus puts strain on the heart
- Thyroid disorders (hyperthyroidism requires an increased level of oxygen to the body)
- Emphysema
Consequences of Congestive Heart Failure: Symptoms of heart failure can begin slowly, so that they are only noticeable at first when a person is active. Then over time, breathing problems and other symptoms will be experienced while at rest. On the other hand, heart failure can also occur suddenly after a heart attack or other physical ailment which significantly impairs heart function.
Symptoms will vary among individuals according to which part of the heart has been weakened and how far along the disease has progressed. But left untreated, worsening congestive heart failure will eventually affect virtually every organ within the body.
While by no means all inclusive, here is a listing of the more common symptoms of heart failure. A number of them are non-specific, which means they are general enough to apply to any number of conditions and thus are necessarily not indicative of heart failure when they are the only symptom experienced. For example, general fatigue could be due to any number of issues, including fighting a cold or other virus, mental stress or a chronic sleep deficiency.
Common symptoms of heart failure:
- General fatigue, weakness or feeling faint
- Dyspnea (shortness of breath), particularly when exercising
- Orthopnea (increasing breathlessness on lying flat)
- Tachypnea (increased rate of breathing)
- Chest working harder to breathe
- Neck veins sticking out
- Coughing
- Cardiac asthma or wheezing (as the disease progresses)
- Rattling or cackling sound when breathing (initially audible only through a stethoscope, indicative of lungs being filled with fluid)
- Cyanosis (skin is bluish or purplish, indicating tissues near the surface of the skin are low on oxygen, occurring in later stages)
- A pulse that feels fast or irregular, or a sensation of feeling the heart beat (palpitations)
- Swelling of the legs and feet (due to fluid accumulation in the body)
- Swollen (enlarged) liver or abdomen (due to fluid accumulation)
- Waking up in the night gasping for breath (due to fluid accumulation in the lungs)
- Only being able to sleep sitting upright (in severe cases of fluid accumulation)
- Increased urination, particularly at night (occurs when fluid from the legs is returned to the bloodstream while lying down)
- Nausea, abdominal pain and decreased appetite (due to fluid accumulation in the liver and intestines)
- Dizziness, confusion and cool extremities at rest (due to poor systemic circulation)
- Weight gain (due to fluid retention)
- Diminished kidney function (poor blood supply to the kidneys prevents them from filtering salt and water from the body)
- Diminished liver function and jaundice (poor blood supply reduces the liver’s ability to rid the body of toxins and produce essential proteins)
- Coagulopathy (decreased blot clotting) (due to diminished liver function)
Left untreated, congestive heart failure will slowly worsen until lack of oxygen eventually causes either the heart or another vital organ to shut down, resulting in death for the individual.
Prevention/management: Since congestive heart failure is a progressive disease for which there is no known cure, the best method of prevention is a healthy lifestyle that includes appropriate food choices, weight control, moderate exercise and adequate sleep. Keeping your body healthy is the best way to protect yourself from this debilitating affliction.
Should you be diagnosed with congestive heart failure, there are ways to manage it. Provided the appropriate lifestyle changes and medication protocol are in place, the majority of individuals can maintain an active, fulfilling lifestyle. However, periodic episodes where a person may need prompt medical attention are not unusual. How often will depend on the nature of the underlying disease, response to medications, severity of any accompanying conditions and individual symptoms experienced.
One very important issue in congestive heart failure is risk of arrhythmias (heart rhythm disturbances), as according to MedicineNet.com, 50% of all deaths in congestive failure patients are related to serious arrhythmias.
Because this congestive heart failure manifests differently from individual to individual, your physician will need to thoroughly understand the nature of your progressive heart failure and develop a unique treatment program targeted specifically for your needs. This program may include any of the following:
- Addressing potentially reversible factors
- If your congestive heart failure has been precipitated by another issue, such as high blood pressure or excess alcohol consumption, getting it under control will help get the congestive heart failure under control.
- If there are other diseases such as diabetes occurring simultaneously with the congestive heart failure, addressing and controlling them may help slow, stop or partially reverse progression of the congestive heart failure.
- Lifestyle changes
- Keep your weight under control, to reduce the stress on your heart and circulatory system.
- Limit your salt intake as much as possible, to help prevent fluid from accumulating in body tissue. An intake no greater than 2000 milligrams per day is often recommended. (The average American “no salt added” diet can contain 4000-6000 milligrams of sodium.)
- Restrict fluid intake, also to help prevent fluid accumulation. Patients with advanced cases are generally advised to restrict total daily fluid intake to no more than 2 litres, even if taking diuretics. Too much fluid can impair the effectiveness of diuretic medication.
- Light exercise, as authorized by your physician. Once discouraged, light aerobic exercise has been shown to maintain overall functional capacity and quality of life, as well as possibly improve survival rates. However, exercise should only be undertaken once one’s heart condition is considered stable.
- Refrain from smoking.
- Limit your alcohol intake, or avoid it all together if alcohol has been a contributing factor to your congestive heart failure.
- Medication – varies by individual, depending on the nature of the heart failure
- Diuretics (water pills), to remove excess fluid from the body by promoting the flow of fluid through the kidneys. (Known side effects: dehydration, electrolyte abnormalities, low potassium levels, hearing disturbances, low blood pressure.)
- ACE (angiotensin-converting enzyme) inhibitors, to help block a hormone (angiotensin II) which can cause problems in people with congestive heart failure. ACE inhibitors have been shown to prevent heart failure and heart attacks. (Known side effects: nagging, dry cough, low blood pressure, worsening kidney function and electrolyte imbalances, and rarely, allergic reactions.)
- ARBs (angiotensin receptor blockers), to do the same job as ACE inhibitors when ACE inhibitors can’t be tolerated. (Similar side effects as ACE inhibitors.)
- Beta-blockers, to block hormones which stimulate more forceful contraction of the heart, which can be detrimental to congestive heart failure patients over the long term. Shown in studies to work well with ACE inhibitors. Should not be used for individuals with asthma, emphysema, or very low resting heart rates. (Known side effects: fluid retention, low blood pressure, low pulse, general fatigue and light headedness.)
- Vasodilators, blood vessel relaxing medications to make it easier for the heart to pump. (Known side effects: chest pain, dizziness, flushing, headache, fluid retention, rapid heartbeat or palpitations, nausea, sinus congestion, racing pulse, vomiting, bloating, sore throat, joint pain, swollen feet or legs, swollen lymph nodes, fever, skin blisters, itching, rapid hair growth.)
- Digoxin, to help the heart contract with more force and provide additional protection against further heart failure, although exactly how is not very well understood. A natural derivative of the Foxglove plant. (Known side effects, but usually only at toxic levels: nausea, vomiting, heart rhythm disturbances, kidney dysfunction and electrolyte abnormalities.)
- Surgery
- Repair of a congenital heart defect or damaged heart valve can arrest the progression of congestive heart failure.
- Coronary bypass surgery and/or angioplasty may help improve blood flow to the damaged or weakened heart muscle.
- Heart transplant for patients whose condition continues to deteriorate. Generally not viable for individuals over 70 or those who have severe or irreversible diseases affecting other organs. Usually done as a last resort as there is significant risk of infection and/or rejection of the transplanted heart.
- Assistive devices
- Sometimes a viable option when heart transplant is not.
- Pacemaker to ensure the heart continues to beat at a regular rhythm.
- Mechanical pump or ECMO (extracorporeal membrane oxygenator) to temporarily improve heart pump function.
- Defibrillator to send an electrical pulse to stop life-threatening abnormal heart rhythms.
- Radiofrequency ablation, to correct abnormal heart rhythm through use of radio waves.
Additionally, a number of other potential treatments are now under study, including new classes of medications (calcium sensitizing agents, vasopeptidase inhibitors, natriuretic peptides) and gene therapy targeted towards certain genes thought to contribute to heart failure.
The prognosis for congestive heart failure is much better than it used to be, and not surprisingly, closely tied to functional classification (see Definition section above). If the underlying condition is caught and treated early enough, spontaneous improvement is often observed, sometimes to the point where heart function becomes normal.
Regardless of the treatment program your doctor has designed for you, there are steps you can take at home to proactively monitor your condition and know when to seek medical attention. Watch for changes in your heart rate, pulse, blood pressure and body weight. Swelling or weight gain of a few pounds over only a day or two can indicate your body is holding onto extra fluid, which could mean your congestive heart failure is getting worse. Go straight to the hospital emergency room or call 911 if you experience fainting, fast and irregular heartbeat and/or severe crushing chest pain.
Do not take drugs or herbs without consulting your doctor. This includes Ibuprofen (Advil, Motrin), Naproxen (Aleve, Naprosyn), Sildenafil (Viagra), Tadalafil (Cialis) and Vardenafil (Levitra).
Additional information: Wikipedia MedicineNet.com PubMed Health Heart.org eMedicineHealth
|
 |
Definition: A slow-developing lung disease which makes it hard to breathe, because the airways are partially obstructed. The air sacs (alveoli) at the end of each airway inside the lungs lose their elasticity and therefore can’t transfer air to and from the lungs efficiently. In addition, the cells in the airways generate more mucous, which clogs them up. Because COPD develops slowly, it can be years before symptoms become significant enough to allow diagnosis of the disease and therefore most people diagnosed with COPD are over 40. Key symptoms include: a cough that doesn’t go away, coughing up excess mucus, shortness of breath (especially with exercise), wheezing and chest tightness.
Known or suspected causes: Smoking (cigarettes, pipes, cigars or other), exposure to second hand smoke or breathing other kinds of irritants such as pollution, dust or chemicals over an extended period of time. In rare cases COPD can be caused by a genetic disorder which results in a deficiency of a liver protein that blocks the destructive effects of certain enzymes. People who have had frequent and/or severe lung infections, particularly as children, also have a greater risk of developing COPD later in life.
Consequences of Chronic Obstructive Pulmonary Disease: There is no known cure for COPD and therefore symptoms will worsen over time – the speed at which this happens will depend on each individual and the degree to which they proactively manage their situation. Death will eventually occur when the heart and lungs are unable to adequately oxygenate the body’s organs and tissues. Individuals with COPD are more susceptible to lung infections, which can be fatal.
Prevention/management: Avoid both smoking and breathing second hand smoke, as well as other lung irritants such as pollution, dust, and certain types of cooking or heating fumes. Remain indoors when outside air quality is poor. Bronchodilators and glucocorticosteroids can help people with COPD breathe easier. As symptoms worsen, portable oxygen tanks can help get more oxygen into the body. In some cases surgery to remove badly damaged areas within the lungs can help ease symptoms, at least on a temporary basis. A lung transplant may be the only survival option for severe cases of COPD.
Additional information: National Heart Lung and Blood Institute
According to the National Heart Lung and Blood Institute (from which the majority of this write up on COPD is based), COPD is the fourth leading cause of death in the US. Most people with COPD also have emphysema and chronic bronchitis. Emphysema is where the walls between the alveoli are destroyed, creating less surface area where air can be transferred in and out of the lungs and causing shortness of breath. Chronic bronchitis is where the airways become inflamed so that excess mucus is produced, leading to constant coughing and further difficulties in getting air in and out of the lungs.
The following illustration, taken from the National Heart Lung and Blood Institute, shows the difference between healthy and damaged lungs:
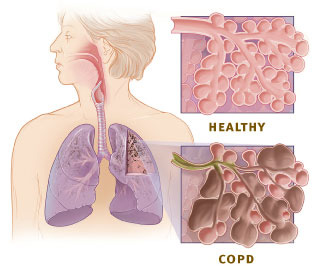
|
 |
Definition: A narrowing or blockage of the coronary arteries (the blood vessels which supply blood directly to the heart) through the build up of plaque. (Plaque is composed of fat, cholesterol, calcium and other substances in our blood.) The blockage restricts blood flow so that oxygen is unable to reach the heart and then portions of the heart start to die. Plaque also increases the risk of blood clots within our arteries. Coronary artery disease is the most common form of heart disease.
Known or suspected causes: Known factors include high blood pressure, unhealthy cholesterol levels, smoking, insulin resistance and diabetes, metabolic syndrome, being overweight or obese, physical inactivity, age and family history.
Other suspected causes currently being studied include high levels of C-reactive protein (CRP) in the blood (occurs when there is inflammation within the body), high levels of triglycerides (particularly for women), sleep apnea, stress and alcohol.
Consequences of Coronary Artery Disease: Angina, heart attack, heart failure or arrhythmias.
Angina is caused by insufficient oxygen getting to the heart and symptoms include a feeling of pressure or squeezing in the chest. Pain can also occur in shoulders, arms, neck, jaw or back.
A heart attack occurs when oxygen to the heart is cut off completely and portions of the heart start to die. Treatment must be immediate to avoid permanent damage to the heart. Without treatment a person could die, depending on the severity of the heart attack.
Heart failure develops over time. The heart becomes unable to pump enough blood throughout the body, either because it can't fill with enough blood or it can't pump the blood with enough force. Although there is no cure, if diagnosed early enough treatment can prolong both life and quality of life. Treatment generally includes both medication and lifestyle changes.
Arrhythmias are problems with the speed or rhythms of the heartbeat. The heart can beat too fast, too slow or irregularly. Most arrhythmias are harmless, but if they prevent an adequate supply of oxygen from circulating within the body, brain and other organ damage can occur.
Prevention/management: Control the risk factors listed above to the best of your ability. Basically, consume a healthy diet, exercise regularly, drink alcohol in moderation and don't smoke.
Additional information: Heart and Stroke Foundation of Canada, National Heart Lung and Blood Institute (US site)
|
 |
Definition: An inflammatory bowel disease (IBD) causing chronic inflammation (swelling) of the lining of the digestive (gastrointestinal) tract, resulting in pain and diarrhea. Crohn’s disease can affect any area of the gastrointestinal tract from mouth to anus, but most commonly affects the lower part of the small intestine (ileum), or the large intestine (colon). Because the immune system plays a key role, Crohn’s disease is also known as an autoimmune disorder.
Because the symptoms of Crohn’s disease are similar to other intestinal disorders such as ulcerative colitis and irritable bowel syndrome (IBS), it can be difficult to diagnose and consequently up to 10% of cases are labeled indeterminate colitis. But whereas ulcerative colitis causes inflammation and ulcers in the top layer of the lining of the large intestine, Crohn’s disease can involve all layers of the intestine and normal healthy tissue can be found between sections of diseased tissue.
The most common symptoms of Crohn’s disease are abdominal pain (often in the lower right area) and diarrhea. Other symptoms may include rectal bleeding, weight loss, arthritis, skin problems, fever and fatigue. Range and severity of symptoms will vary by individual.
Symptoms and complications will also vary depending on which part of the intestinal tract is inflamed:
- Ileocolitis – Most common form (50% of cases), affecting both the ileum (small intestine) and colon (large intestine). Symptoms include diarrhea and cramping in the lower right or middle parts of the abdomen, often accompanied by significant weight loss.
- Ileitis – Affects the ileum only (30% of cases). Symptoms are the same as Ileocolitis and complications may include fistulas or inflammatory abscess in the right lower quadrant of the abdomen.
- Crohn’s colitis – Affects the colon only (20% of cases). Symptoms include diarrhea, rectal bleeding (bloody diarrhea), and disease around the anus (abscess, fistulas, ulcers). Skin lesions and joint pains are most common in this form of Crohn’s disease.
Known or suspected causes: Although several theories exist regarding the cause of Crohn’s disease, none of them has been proven correct. Current thinking is that the body’s immune system somehow malfunctions and starts seeing food, bacteria and other substances as foreign bodies that need to be attacked. The resulting high level of white blood cells in the intestinal area creates excessive swelling, ulceration and injury, causing pain, diarrhea and the other complications listed below.
Some reports indicate this disease appears to affect women more than men, and although it can appear at any age it is most commonly diagnosed between the ages of 15-30. About 20% of people with Crohn’s disease have a blood relative with some form of inflammatory bowel disease, suggesting a hereditary factor. In fact, parents, siblings or children of people with Crohn’s disease are 3-20 times more likely to develop the disease and twins have a 55% probability.
People of Jewish heritage are at increased risk, while African Americans are at decreased risk.
Individuals living in developed countries, specifically the US and Europe, are at greater risk of developing the disease, which is more common in northern countries and in urban centres versus more rural areas.
Consequences of Crohn's Disease: The most common complication is blockage of the intestine as ongoing swelling and accumulated scar tissue narrows the passage. Symptoms include crampy pain around the mid-abdomen and vomiting, as well as bloating and distention.
In about 30% of cases, sores or ulcers can migrate to surrounding tissues such as the bladder, vagina and skin, as well as rectum or anus. The migration could lead to tunnels or fistulas that become infected and possibly require surgery. Small tears called fissures may develop in the mucus membrane of the anus. Serious or persistent bleeding could lead to anemia.
Children with Crohn’s disease may suffer delayed development or stunted growth.
Nutritional deficiencies caused by inadequate dietary intake, intestinal loss of protein and poor absorption are common. A depressed appetite can interfere with adequate dietary intake, especially during flare ups, since chronic diseases tend to increase the caloric needs of the body.
Other complications include arthritis, skin problems, inflammation in the eyes, mouth or low back/spine, kidney stones, blood clots, gallstones or other diseases of the liver and biliary system (including liver failure), which may either resolve during regular treatment for the Crohn’s condition or require separate treatment.
Neurological complications, such as seizures, stroke, myopathy, peripheral neuropathy, headache and depression, can be present in up to 15% of cases.
Massive distention or dilation of the colon and rupture of the intestine are both potentially life threatening situations requiring surgery, but fortunately both events are rare occurrences.
Recent data suggests there may be an increased risk of colon cancer in patients with long-standing Crohn’s disease.
In addition, people with Crohn’s disease often experience a great deal of stress while having to cope with a chronic disease. However, most are able to hold jobs, raise families and function successfully in society, despite ongoing medication and the occasional hospitalization.
Prevention/management: Management may include drugs (anti-inflammatories, corticosteroids, immune modifiers, antibiotics, anti-diarrheal and fluid replacements, biologic therapies (new drugs that block immune function so that inflammation does not occur), nutrition supplements (sometimes intravenously if the intestines need a rest) or surgery (when medications no longer control symptoms), or a combination of these options. Because there is no cure, treatment focuses on controlling inflammation (so that tissues can heal), correcting nutritional deficiencies and relieving symptoms like pain, diarrhea and rectal bleeding. Treatment depends on the location and severity of the disease, which may go into remission for years but almost always recurs at some point.
There is no supplement or diet proven to prevent or control Crohn’s disease, but sufferers should take care to follow a nutritious diet and avoid foods which appear to worsen symptoms. Though their ability to absorb necessary nutrients is compromised, people with Crohn’s disease should take vitamin supplements only on their doctor’s advice.
Abdominal discomfort and cramping can be minimized by eating smaller meals at more frequent intervals, reducing the amount of greasy or fried foods within one’s diet, limiting consumption of milk or milk products if lactose intolerant and restricting intake of high fibre foods such as nuts, seeds, corn , popcorn and various Chinese vegetables if narrowing of the bowel is suspected; these foods can also cause diarrhea if they enter the large intestine only partially digested. A low fibre, low residue diet can help with pain and cramping, but this limits variety and makes it difficult to ensure adequate intake of all one’s nutritional needs. Common deficiencies include vitamin B-12, folate, vitamin D, calcium, potassium and magnesium. Iron deficiency can also occur from blood loss due to inflammation and ulceration of the colon. Deficiencies experienced by each individual are dependent on which part(s) of the gastrointestinal tract are afflicted.
Because of the ongoing diarrhea, people affected by Crohn’s disease can become severely dehydrated and so should consume one half ounce of water per day for every pound of body weight. Water should be sipped rather than gulped to avoid the discomfort of additional air within the digestive system.
Two thirds to three quarters of all individuals suffering from Crohn’s disease will require surgery at some point and often more than once. Removing the affected area within the intestines can help but is not considered a cure since the disease generally migrates to the area next to where the diseased tissue was removed. In severe cases the entire colon may be removed via colectomy and a pouch to collect waste attached for patients to empty as needed.
Additional information: National Digestive Diseases Information Clearinghouse, Crohn's & Colitis Foundation of America, Medicine Net, Wikipedia
|
 |
Definition: A chronic metabolic disorder characterized by elevated levels of blood glucose (blood sugar). In a normally functioning person, the pancreas works to keep blood sugar levels within a fairly narrow range by producing insulin to reduce blood sugar levels after eating (insulin enables sugar to be absorbed into liver and muscle cells) and glucagon to increase blood sugar levels once they fall too low (glucagon directs the liver to produce glucose). In a person with diabetes, the pancreas is either unable to produce insulin or can not produce a high enough level of insulin to lower blood sugar to a safe range.
There are different forms of diabetes:
- Type 1 Diabetes (formerly known as Childhood-Onset Diabetes, Juvenile Diabetes or Insulin Dependent Diabetes) – may be caused by the body’s immune system attacking and destroying insulin-producing cells. It usually develops in children and adolescents (around puberty) and in rare cases, adulthood. This is an inherited disease most commonly found in northern Europeans. About 10% of all diabetes cases are of this type.
- Type 2 Diabetes (formerly known as Adult-Onset Diabetes, Obesity-Related Diabetes or Insulin Resistant Diabetes) – caused by the body’s cells becoming resistant to insulin so that more and more insulin is required for cells to absorb glucose. When the pancreas can no longer keep up with the rising demand for insulin, blood sugar levels rise and diabetes develops. 90% of diabetes cases are type 2.
- Gestational Diabetes – similar to type 2 diabetes, occurring temporarily during pregnancy and disappearing after childbirth (although 20-50% of women afflicted go on to develop type 2 diabetes later on in life and risk of childhood obesity and type 2 diabetes later in life is higher for their children). It is thought that hormones produced by the placenta affect the action of the mother’s insulin. Gestational diabetes occurs in approximately 2-5% of all pregnancies.
- Other – caused by diseases (i.e. pancreatitis, pancreatic cancer) or chemicals (i.e. hemochromatosis) which destroy the pancreas. Surgical removal of the pancreas can trigger type 1 diabetes, while some medications (i.e. corticosteroids, diuretics, beta blockers) can increase insulin resistance and cause type 2 diabetes.
Diabetes has rapidly become a worldwide epidemic. Approximately 3 million Canadians and 8% of Americans have diabetes. Diabetes has become a worldwide epidemic - current estimates are that globally 246 million people have diabetes and that the total number is projected to reach 380 million within the next 20 years. The rapid growth of type 2 diabetes in Canada is due in large part to the following: an aging population, rising obesity rates, increasingly sedentary lifestyles and immigration (almost 80% of new Canadians come from populations at higher risk for type 2 diabetes – Hispanics, Asians, South Asians or Africans).
Known or suspected causes: As noted above, type 1 diabetes is caused by a malfunction in the body’s immune system and is hereditary in nature, although there is some evidence to show an environmental trigger is required. Type 1 diabetes may be triggered by viral infections, stress or exposure to certain chemicals or drugs.
Type 2 diabetes is caused by insulin resistance; when the pancreas can no longer keep up with the body’s increasing demand for insulin, diabetes develops. Risk factors for type 2 diabetes include family history of diabetes (more so than for type 1 diabetes), being of Aboriginal, Hispanic, Asian, South Asian or African descent, being overweight (particularly if most of the weight is around the middle section of the body), currently experiencing health complications associated with diabetes, impaired glucose tolerance or impaired fasting glucose, high blood pressure, high cholesterol or other fats in the blood, polycystic ovary syndrome, acanthosis nigricans (darkened patches of skin due to insulin spillover) or schizophrenia. Additional risk factors for women include having given birth to a baby that weighed over 4 kg (9 lb) at birth or having had gestational diabetes (diabetes during pregnancy).
Consequences of Diabetes Mellitus: The symptoms of high blood sugar, or hyperglycemia, are similar regardless of diabetes type, and include blurry vision, excessive thirst, frequent urination, feeling very hungry or tired, weight gain or loss (without trying), frequent or recurring infections, cuts and bruises that are slow to heal and tingling/numbness in the hands or feet.
With type 1 diabetes, symptoms are noticeable almost immediately, within days or weeks. However, type 2 symptoms develop gradually and can therefore be overlooked, so that it takes an average of 9-12 years to be diagnosed. The Canadian Diabetes Association recommends that people over 40 be tested for diabetes on a regular basis, and that those under age 40 be tested if there is family history.
Many individuals are at the "prediabetes" stage (also known as borderline diabetes, impaired glucose tolerance or impaired fasting glucose), where blood glucose levels are above normal but have not yet reached the diabetes level. Although not everyone will go on to develop type 2 diabetes, many will if steps are not taken to reduce blood glucose levels with lifestyle changes (diet and exercise). Some long term complications of diabetes such as heart disease and nerve damage may begin during the prediabetes stage.
If left unchecked, diabetes can lead to hyperglycemia, ketoacidosis or hypoglycemia, and over the longer term, blindness, kidney failure and heart disease (3 out of 4 people with diabetes die from heart disease or stroke). Diabetes can also cause nerve damage and impair circulation, which impedes natural healing capacity and ability to fight infection. Nerve damage can also lead to changes in sensory perception and problems with digestive, bladder, bowel or sexual function. Serious nerve damage, especially when combined with poor circulation, can lead to foot ulcers (loss of sensory perception means that pain is not felt and so the ulcers can go unnoticed until it’s too late because the ulcer has penetrated to the bone or gangrene has set in) and the loss of lower limbs (particularly the toes).
Hypoglycemia, or low blood sugar, is most common in type 1 diabetics, but it can occur with type 2 diabetes and if not recognized can be life threatening. Blood sugar can fall to abnormally low levels from too much insulin, too much exercise, too little food or carbohydrates, a missed or delayed meal or a combination of these factors. Symptoms include nervousness, weakness, hunger, dizziness, trembling, sweating, rapid heartbeat, feeling cold and clammy, irritability, confusion, drowsiness, slurred speech, double vision and in severe cases, loss of consciousness, seizures and eventually diabetic coma. Alcohol consumption can be a contributing factor to hypoglycemia, particularly if one is taking insulin or oral diabetes medication. See my article Alcohol: How Much Is Too Much? for details. Important information about the diabetes/alcohol relationship is available on Beachway Therapy Center's web site.
People with diabetes are at greater risk for cavities and other types of dental problems, including oral fungal infections, because elevated blood sugar allows bacteria to thrive in the mouth, leading to tooth decay and possibly to increased risk and severity of gum disease. Good dental hygiene and regular dental visits are therefore imperative.
Infections and other illnesses cause the production of stress hormones that counteract insulin. It is therefore especially important to monitor blood sugar levels when feeling under the weather.
There is some risk to both mother and child during pregnancy. Diabetic problems experienced before pregnancy tend to worsen during pregnancy but the damage often reverses after delivery. The best thing a woman can do to maximize the chances of a healthy pregnancy for both herself and her baby is ensure her blood sugar level is under control before getting pregnant and keeping it that way throughout the pregnancy. Consistently high levels of blood glucose increase the chances of miscarriage or premature labour. Babies tend to be larger but there is a risk of immature lungs or low levels of calcium or glucose at birth. There is also higher risk of organ deformation in the fetus, including neural tube defects (incomplete development of the brain or spinal cord), anencephaly (absence of the brain or spinal cord) and spina bidfida (failure of the backbone to fuse over the spinal cord).
Prevention/management: A healthy diet, weight control, not smoking and physical activity are all key to the delay or prevention of type 2 diabetes.
There is no definitive cure for either type 1 or type 2 diabetes, although pancreas or pancreas-kidney transplants have "cured" some people with type 1 diabetes. A certain type of gastric bypass surgery has normalized blood sugar levels in the majority of patients although no one is certain why and so it is being studied intensely. Other forms of research are underway for type 1 diabetes that attempt to get the body producing insulin once again, and some of the results to date appear quite promising.
Both types 1 and 2 diabetes can be managed to dramatically reduce the risk of serious long term complications. The goal of treatment is to keep blood sugar levels as close to normal as possible to prevent damage to eyes, kidneys, heart, nerves and blood vessels. This means understanding the impact of specific foods on one’s blood sugar levels and then matching insulin delivery to insulin requirements (largely a function of meal size and content). Monitoring blood sugar levels regularly teaches a person how certain foods affect their glucose level production so that diet (and timing/amount of daily insulin injections, if required) can be fine tuned to their specific needs. Monitoring blood sugar on an ongoing basis before and after specific activities (or when one experiences some of the symptoms of hypoglycemia noted above) can also help guard against hypoglycemia.
Specific treatment for type 1 diabetes focuses on supplying the body the insulin it can’t produce on its own.
Treatment for type 2 diabetes includes diet, exercise and possibly medication to overcome the insulin resistance. However, insulin injections often become necessary.
Regardless of which type of diabetes is involved, a diet low in saturated fats and high in fibre, fruits and vegetables is recommended to both lower blood sugar levels and reduce the risk of cardiovascular disease. Daily protein requirements should be obtained from beans, grains and vegetables rather than meat to keep fat and cholesterol intake kept to a minimum.
While proteins, fats and carbohydrates all trigger glucose production, carbohydrates contribute to most of the glucose produced after a meal. The amount of glucose produced and the speed at which it enters one’s system varies by food type. The majority of carbohydrate intake should be complex carbohydrates in the form of vegetables, whole grain breads and cereals, because complex carbs digest more slowly and therefore lower the speed at which glucose is released into the system. Raw vegetables are digested more slowly than cooked ones, an apple is digested much more slowly than apple juice and eating fats with carbohydrates also retards digestion.
Artificial sweeteners don’t raise blood glucose levels and so are a good substitute for table sugar, which is dangerous in large amounts due to the rapid spike in glucose created upon ingestion. This results in too much sugar in the urine, which inhibits the kidneys from reabsorbing water. The required water is then removed from body cells, causing dehydration and increased thirst. Although rare, this can lead to diabetic coma.
Alcohol is a carbohydrate and if one chooses to drink must be counted as part of the total carbohydrate intake for the day. Be aware that some symptoms of intoxication (i.e. drowsiness and slurred speech) are similar to symptoms of hypoglycemia (low blood sugar) and so a true diabetic emergency might not be immediately recognized.
While regular exercise is important to weight loss, protection against heart disease and overall good health, exercise consumes glucose and can therefore cause low blood sugar, leading to severe hypoglycemia. Therefore, exercise under doctor supervision, wear a medical alert bracelet and keep hard candy or glucose tablets available in case blood sugar drops significantly. Those who take insulin should check their blood sugar level before starting to exercise.
To guard against diabetes-related complications, people with diabetes should see their doctor regularly and have their blood pressure, blood lipid levels and kidney function checked frequently, as well as have their feet examined. An annual eye examination by an ophthalmologist is also recommended, since diabetes is the leading cause of blindness in people aged 20-74 (through retinopathy, the development of cataracts or glaucoma).
Additional information: Canadian Diabetes Association, American Diabetes Association, Wikipedia, Everyday Health
|
 |
Definition: One of the most common causes of pelvic pain and infertility in women, endometriosis is a condition where tissue similar to the lining of the uterus (shed each month during menstruation) is found elsewhere in the body. This endometrium tissue can be found anywhere in the pelvic cavity – on the ovaries, the broad ligaments (beneath the ovaries), the fallopian tubes, the pelvic sidewall, the uterosacral ligaments, the Pouch of Douglas and/or the rectovaginal septum. Less common locations include caesarian-section scars, laparoscopy or laparotomy scars, bladder, bowel, intestines, colon, appendix or rectum. In rare instances, endometriosis has been found in the kidney, in the bladder, in the diaphragm, on the skin, in the lung, in the spine and even inside the brain.
Wikipedia estimates endometriosis occurs in 5-10% of women.
Known or suspected causes: The cause of endometriosis is unknown, although several theories do exist. However, studies have shown that there is a hereditary link and that the disease tends to be worse in the next generation.
Consequences of Endometriosis: The most common symptom is pelvic pain, which can be severe enough to significantly affect lifestyle and quality of life. The pain often, but not always, corresponds to the menstrual cycle. Because symptoms are “invisible” (i.e. no one else can “see” the pain), family and friends may not understand the degree of pain and fatigue being experienced.
Pain may be felt before/during/after menstruation, during ovulation, in the bowel and/or lower back during menstruation, when passing urine, during bowel movements, during or after sexual intercourse and/or in the lower back area.
Other symptoms may include diarrhea or constipation (particularly in connection with menstruation), abdominal bloating (again, in connection with menstruation), nausea, vomiting, urinary urgency or frequency, short menstrual cycles, heavy or irregular bleeding (sometimes severe enough to require iron supplements or blood transfusions), mood swings and/or fatigue.
In more severe cases, scar tissue and adhesions (fibrous bands of scar tissue that bind internal organs together ) can distort the internal anatomy. Bowel or uterine obstructions can occur from pelvic adhesions. In advanced stages internal organs may fuse together, causing frozen pelvis. These issues in turn can create even more pain than the endometriosis itself.
On rare occasions, an endrometrionic cyst on an ovary can burst, causing a life threatening infection in the pelvic cavity.
30-40% of women are infertile, making endometriosis second only to pelvic inflammatory disease as the leading cause of infertility in women that ovulate normally. (In fact, endometriosis is suspected to be present in a significant number (20-50%) of infertile women.) Others may have difficulty conceiving due to fallopian tube blockage. Alternatively, pregnancies may result in early miscarriage.
Some experts hypothesize that endometriosis can lead to ovarian or other cancers.
Prevention/management: Ultrasound, MRI scans and gynaecological examinations can neither definitively confirm nor dismiss the presence of endometriosis, so that the only reliable diagnosis test is to take a biopsy of internal tissue via laparoscopy.
Because there is no cure, treatment depends on each woman’s particular symptoms and focuses primarily on relieving pain. Some women experience very little pain despite extensive lesions while others experience intense pain even though they only have a few small areas of endometriosis.
Excess estrogen seems to contribute to endometriosis growth and pain, so treatment often includes hormonal therapies such as continuous oral contraceptives that temper estrogen production and prevent menstruation. Progesterone or progestins (chemical variants of natural progesterone) counteract estrogen and inhibit growth of the endometrium.
When bleeding is excessive, birth control pills, hormone therapies, IUDs with hormones, drugs that induce menopause or even hysterectomy are all possible treatments to stop the bleeding.
Laparoscopic surgery can be used to remove endometrionic cysts, lesions and adhesions.
A hysterectomy and/or removal of the ovaries does not guarantee endometriosis will not come back and is not recommended unless these organs are diseased. Similarly, some women continue to experience endometriosis symptoms after menopause.
Additional information: Canada.com Endometriosis.org Wikipedia
|
 |
Definition: An arthritis related condition characterized by chronic widespread muscle, ligament and tendon pain and painful responses to a usually non-painful stimulus, including tender points particularly sensitive to pressure. Other symptoms may include sleep disturbances, severe fatigue, depression and anxiety, cognitive difficulties, headaches (including migraines), bladder irritability and spasms, irritable bowel syndrome (abdominal pain and bloating with alternating constipation and diarrhea), jaw problems (temporomandibular joint disorder), morning stiffness, tingling or numbness in hands and feet and painful menstruation.
Fibromyalgia affects 900,000 (3 in 100) Canadians with women four times more likely then men to develop the disease, which generally occurs in people over 50. However, younger people, including children, are affected as well.
Known or suspected causes: The cause of fibromyalgia is unknown, but the following have been loosely associated with disease onset: stressful or traumatic events (i.e. physical like car accidents or non-physical emotional turmoil), repetitive injuries, viral infections and genetic predisposition (although no hereditary link has been identified). Some scientists suspect either lack of exercise and changes in muscle metabolism or overuse of muscles may play a role. Sleep disturbances may also play a role, as it lowers production of a growth hormone crucial to repair of muscles.
Consequences of Fibromyalgia: Depression and fibromyalgia tend to go hand in hand, but it’s not known whether depression is a cause or effect of fibromyalgia.
Fibro-fog is the name commonly given to the cognitive problems associated with fibromyalgia, which include confusion, memory lapses, word mixups and difficulty concentrating. Part of the cause of fibro-fog may well be the disturbed sleep patterns experienced by fibromyalgia sufferers.
About 10% of people with fibromyalgia also have restless leg syndrome, which causes their legs to spasm during sleep.
Constantly feeling tired impacts quality of life as it severely limits what one is capable of accomplishing during a typical day. It’s difficult to plan ahead when one isn’t sure how they are going to feel day to day.
Although having fibromyalgia does not increase the risk of developing other diseases, people with autoimmune diseases such as rheumatoid arthritis and lupus are at increased risk of developing fibromyalgia. In fact, 20-30% of people with rheumatoid arthritis also develop fibromyalgia, although the exact connection between the two diseases is unknown.
Despite the widespread pain and discomfort associated with this disease, there is no evidence of inflammation or damage occurring in muscles or internal organs.
Prevention/management: There is no specific lab test for fibromyalgia and the effects on the body are invisible (i.e. there is no swelling or deformation like with other types of arthritis), which makes this disease very difficult to diagnose. In fact, many people who have the fibromyalgia are told their complaints about hurting all over and constantly feeling tired are “all in their head”. The best option therefore is to consult a rheumatologist, a doctor who specializes in fibromyalgia and rheumatic diseases.
Unfortunately, just as there is no test for fibromyalgia, there also is no cure. However, appropriate treatment, regular exercise and healthy lifestyle habits can relieve symptoms and allow most people to lead a fairly normal life.
Treatment generally consists of weight control, moderate exercise, relaxation techniques, a healthy well balanced diet with limited alcohol intake, medications to diminish pain, counter depression and improve sleep, and possibly alternative therapies such as acupuncture, acupressure, yoga, massage or herbs and supplements.
In addition, fibromyalgia sufferers should employ energy saving techniques to reduce fatigue and place less stress on muscles. Combine errands and chores to get more done with less effort, plan simple meals that require little or no preparation, keep shopping short and simple, etc.
Additional information: Arthritis Society of Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Today, Arthritis Foundation, Fibromyalgia Symptoms
|
 |
Definition: A common form of inflammatory arthritis affecting 1 in 30 Canadians, and the most common inflammatory arthritis among men. Unlike most types of arthritis, gout can flare up for days or weeks on occasion before going into “remission”. However, as the disease progresses, gout can also become chronic.
Acute flare ups include mild to excruciating pain, redness, swelling and warmth within the joints, lasting days to weeks. There may also be a feeling of pressure around the joint and a feeling like the skin around the area is stretching or tearing. Most initial attacks occur in the lower extremities, most commonly in the big toe joint. However, the ankle, knee, foot, hand, wrist and elbow joints can also be affected.
The initial onset of gout can be quick and unexpected, and the pain so excruciating that a person is unable to tolerate the pressure of a single bed sheet, let alone wearing shoes. Initial attacks usually involve only one joint and with treatment, the pain tends to subside within 3-10 days.
The good news is that gout is a controllable disease and with proper treatment will not cause any serious long term problems.
Known or suspected causes: Caused by hyperuricemia, which is an imbalance of in the production and excretion of uric acid, a waste product naturally occurring in the body and normally excreted in urine. Hyperuricemia can be either the result of too much uric acid production or not enough excretion.
The resulting imbalance puts too much uric acid in the blood and deposits needle-shaped monosodium urate crystals in tissues and joints, causing debilitating joint pain and inflammation. (There may be periods where there are no symptoms and the disease appears to be in remission, but urate crystals continue to be deposited so that damage is still occurring.)
Risk factors for developing gout include family history, being overweight, hypertension, some medications (i.e. diuretics) which prevent uric acid from leaving the body, alcohol (particularly beer), certain foods (seafood, organ meats, coffee, tea), and events such as strokes, heart attacks or surgery. Sudden dietary changes or rapid weight gain/loss can also trigger gout.
Consequences of Gout: Joint pain can be excruciating and therefore quite debilitating, interfering with quality of life. Without treatment, flare ups will last on average from 7-10 days.
Uric acid crystals can also be deposited in soft tissues and form whitish or yellowish deposits under the skin, known as tophi, causing irritation and redness and which will at times break through the skin. Tophi can occur anywhere but most often shows up in the fingers or toes, at the backs of elbows, behind the heels or around the outer edges of the ears.
People with gout also have an increased risk of kidney stones.
A condition called uric acid nephropathy or gout nephropathy can result in impaired kidney function up to and including kidney failure.
Prevention/management: There is no cure for gout, so the goals of treatment are therefore both pain management and prevention of future attacks and their resulting damage to the joints, as well as to prevent the formation of tophi or kidney stones.
Therapy for acute flares includes nonsteroidal anit-inflammatory drugs, steroids (cortisone) and colchicines, although there are significant side effects associated with this drug.
Heat (relaxes aching muscles and increases circulation but may worsen symptoms) or cold (constricts blood vessels, blocks nerve impulses and decreases inflammation) application can also provide temporary relief of pain.
Diet and lifestyle modifications include weight loss, avoiding alcohol, reducing dietary purine intake, and stopping medication associated with hyperuricemia (i.e. diuretics). Once pain is under control, exercise (range of motion to reduce joint stiffness, muscle strengthening exercises to protect joint, low impact endurance exercises for energy and weight control) will help strengthen and protect the joint. Protect your joints by using them in ways that minimize stress placed on them – use canes, luggage or grocery carts, shoulder bags versus hand held ones, etc.
Additional information: Arthritis Society of Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Foundation
|
 |
Definition: Heart disease is any disorder which affects the heart's ability to function normally, whether that involves the blood vessels which supply blood to the heart, the functioning of the valves inside the heart or the ability of the heart to pump efficiently. Heart disease can develop over time or be present at birth (congenital heart disease).
Known or suspected causes: Coronary heart disease (also known as coronary artery disease and is the most common cause of heart disease), hypertension, abnormal heart valve function, abnormal heart rhythm, weakening of the heart's pumping ability due to infection or toxins.
Consequences of Heart Disease: Heart disease is the number one killer in the US (responsible for over one quarter of all deaths in the US) and a major cause of disability. Symptoms include chest or arm pain or discomfort, shortness of breath, dizziness or nausea, abnormal heartbeat, fatigue or unnatural tiredness.
Prevention/management: Risk increases with age, particularly for men over 45 and women over 55. Risk also increases if a close family member developed heart disease at an early age. To minimize your risk of developing heart disease, you should strive to keep the following under control:
- Blood pressure
- Cholesterol
- Diabetes
- Body weight
- Stress
In addition, avoid smoking and excessive alcohol consumption. Do eat a healthy diet that is high in fruits and vegetables and low in fat (particularly saturated and trans fats). Follow a regular exercise program.
Women face additional risk factors for heart disease. Our higher estrogen levels protect us in our younger years, but as we pass through menopause our estrogen level drops and our risk of heart disease increases substantially. Our cholesterol and triglyceride levels tend to increase and so does our blood pressure. Our ability to handle sugar is reduced, so that we are at higher risk of diabetes. The way our body stores fat and the way our blood clots can also be affected. Therefore it is even more important to maintain a healthy diet and lifestyle as we age.
Birth control pills can increase the risk of high blood pressure and blood clots in a small percentage of women. To be safe, woman who take oral contraceptives should not smoke.
According to the Heart and Stroke Foundation, pregnancy and childbirth can increase the risk of stroke from 3 to 13 times, with risk being the greatest in the six weeks following childbirth.
Additional information: Heart and Stroke Foundation of Canada, Fact Sheet on the Heart Health of Canadian Women
|
 |
Definition: Hepatitis stems from the Greek hepar (liver) and -itis (inflammation) and identifies a medical condition where there are inflammatory cells in the liver. The condition can heal on its own or progress to fibrosis and/or
cirrhosis. Hepatitis can be classified as either acute (lasting less than six months) or chronic (ongoing). Sometimes it clears up on its own and the virus completely disappears from the body, but often the virus remains in the body so that a person becomes a carrier of the disease. With chronic hepatitis, the virus can be either active or inactive within the body at any point in time. Some people feel no symptoms at all, while others experience anything from mild illness to serious liver damage.
Hepatitis can be caused by a number of different factors , including toxic sources (alcohol, certain medications*, some industrial organic solvents and plants) and underlying metabolic conditions (infections and autoimmune diseases), but in common usage it refers to viral hepatitis. While there are five identified hepatitis viruses, the overwhelming majority of cases are caused by three. This article therefore focuses on these three common virus types, known as A, B and C.
*While certainly not an exhaustive list, certain common medications worth noting include amoxicillin, hormonal contraceptives, Loratadine (antihistamine), Ibuprofen and indomethacin (NSAIDs) as well as acetaminophen when overdosed.
- Hepatitis A (HAV – hepatitis A virus) is a highly contagious foodborne and/or waterborne infection causing acute (short term) illness that can take several months to fully heal. It can also be transmitted person to person, notably through oral and anal sexual activity. In most cases, it will clear up without any permanent liver damage. In addition, once you’ve had hepatitis A, your body will develop a natural lifelong immunity so that you will not get it again.
- Hepatitis B (HBV – hepatitis B virus) is also highly contagious (about 100 times more infectious than HIV, the virus which can lead to AIDS). It begins as acute, but for a small percentage of infected people (ranging from 5% to 25%, depending on the source of my research) the virus will remain in the body and cause long term liver problems such as cirrhosis, liver cancer and liver failure. Infants and children are most susceptible to developing chronic hepatitis. With chronic hepatitis B, often no symptoms appear until the liver is severely damaged. However, once identified chronic hepatitis B is treatable.
- Hepatitis C (HBC – hepatitis C virus) is less contagious than hepatitis B since transmission is generally through infected blood only, although it can also be sexual transmitted. The infection can be short term, but 60-75% (depending on the source of the research) of infected people will develop chronic Hepatitis C and are at risk for cirrhosis, liver cancer and liver failure. Like hepatitis B, often no symptoms are experienced until liver damage is severe.
According to a 2013 World Health Organization (WHO) report 2013 World Health Organization report, hepatitis B and hepatitis C together caused 1.4 million deaths in 2010, including deaths from acute infection, liver cancer and liver cirrhosis. WHO estimates that hepatitis B and C viruses are responsible for 57% of liver cirrhosis cases and 78% of primary liver cancer cases worldwide.
One of the reasons why hepatitis B and C are such worldwide epidemics is that symptoms are often silent until substantial and often irreversible liver damage has occurred. Although a vaccine is available for hepatitis B (and also for hepatitis A), at present there is no vaccine available for hepatitis C. WHO estimates that approximately 240 million people worldwide are chronically infected with hepatitis B and 184 million people have antibodies to hepatitis C. (The presence of antibodies will indicate that a person has been exposed to the hepatitis C virus at some point in their lives, but depending on the testing method it may not indicate whether the infection is currently active.)
Health Canada estimates that about 5% of Canadians have had an acute infection of Hepatitis B at some point in their lives, and that 0.7-0.9% of the Canadian population is dealing with chronic Hepatitis B. The Canadian Liver Foundation estimates that approximately 250,000 Canadians have Hepatitis C, and many don’t know they’re infected (as well as infectious to others) because it can take up to 20 or 30 years before they feel sick.
Known or suspected causes:
Hepatitis A
According to the US Center for Disease Control (CDC), there are two main sources of exposure to hepatitis A:
- Person-to-person transmission through the fecal-oral route, or ingestion of something that has been contaminated with the feces of an infected person or animal. Most infections in the US result from close personal contact with an infected household member or sex partner.
- Exposure to fecally contaminated food or water. Exposure to HAV-contaminated food can lead to both individual and localized group outbreaks. Although the virus can be killed by heating food greater than 85° C (185° F), it can still be spread from cooked food if the food is contaminated after cooking. Contaminated fruits and vegetables in grocery stores and infected food-handlers who do not wash their hands properly after using the washroom are potential sources of contamination. Waterborne cases are rare in developed countries with well-maintained sanitation and water supplies, since adequate chlorination kills the virus.
The hepatitis A virus can live outside the body for months, depending on environmental conditions. It is therefore important to ensure good sanitary practice in your kitchen by adequately washing all fruits and vegetables, fully cooking foods (particularly shellfish and other seafood) and ensuring countertops and cooking utensils are properly cleaned after use.
Precautionary care should be taken if you are living with someone who is newly infected with hepatitis A or when traveling to areas where the virus is common (e.g. The Caribbean, South America).
Hepatitis B and C
Hepatitis B is transmitted through contact with body fluids such as blood, semen, vaginal fluids and wound exudates (clear or pus-like fluids that ooze from cuts or from areas of infection or inflammation). It can also be transmitted through saliva, although the concentration of the virus in saliva is much less than in blood or semen, so that transmission is rare if blood is not visibly evident in the saliva.
Hepatitis C transmission occurs through blood to blood contact only, making it less contagious than hepatitis B.
High risk factors for both include:
- Sex with an infected partner, or sex with multiple partners
- Oral sex with an infected partner (primarily for hepatitis B, there is lesser risk for hepatitis C unless blood is present)
- Injection drug use that involves sharing needles, syringes or other drug paraphernalia equipment
- Being born to a hepatitis B infected mother
- Contact with blood or open sores of an infected person
- Tattoos, piercings, manicures, pedicures and medical or dental procedures with improperly sterilized equipment
- Sharing items such as razors, scissors, nail clippers or toothbrushes with an infected person
- Blood transfusions or organ transplants using inadequately screened blood products
- Providing emergency first aid where you come in contact with blood or other body fluids
Neither virus is spread through food or water, sharing food, drinks or eating utensils, coughing or sneezing, toilet seats, breastfeeding (unless the nipples are cracked and bleeding), hand shaking or hand holding, hugging, dry kissing, or other casual contact.
Since the hepatitis C virus can survive outside the body up to 4 days and the hepatitis B virus can survive at least 7 days, it is important to wear gloves when cleaning up blood spills (wet or dry) and to thoroughly disinfect the area using at least one part bleach to 10 parts of water.
Consequences of Hepatitis:
Hepatitis A
Most hepatitis A infections are acute, in that they last for a limited time period before the body heals itself. Some people feel nothing at all, while others experience only vague, flu-like symptoms. More severe symptoms may include fatigue, muscle and joint aches, headache, nausea and vomiting, abdominal discomfort, diarrhea, grey coloured stool, jaundice (yellowing of the whites of the eyes and skin caused by waste that the liver hasn't been able to process), dark urine, low grade fever and poor or complete loss of appetite. There may be some physical swelling of the liver.
Age is a factor in determining severity of symptoms. In general, children will have milder symptoms than adults, and the older you are the more severe your symptoms are likely to be. Symptoms may appear anywhere from 15 to 50 days after being exposed to the virus, and last from one or two weeks to several months.
Most of the time there are no long term consequences, although acute cases have been known to progress to liver failure, particularly for people who have pre-existing chronic liver disease, including chronic hepatitis B or C.
It is important to know that infected individuals can still transmit the virus to other people, even if they aren’t experiencing any symptoms.
Hepatitis B
Like hepatitis A, hepatitis B will begin as an acute infection and symptoms may be vague to non-existent. Most adults with a properly functioning immune system (75%) will clear the infection completely. However, babies and children are more likely to become carriers of hepatitis B for life even if they experienced no symptoms at the acute stage, because their less developed immune system is unable to fully clear the virus from their body. With children, chronic infections often go undetected until much later in life when as an adult they become seriously ill with liver disease.
Even if the acute infection progresses to chronic, only about one in four individuals with chronic hepatitis B will have active disease that may lead to cirrhosis, liver failure or liver cancer. As long as a person’s immune system remains strong they will be able to keep their infection in remission, but it could become active if their immune system does become compromised by another viral infection, invasive medical procedures like chemotherapy, high stress levels, and so on. Ongoing active disease will require treatment to protect liver function.
Extensive liver damage to the point of cirrhosis is characterized by jaundice, weight loss, easy bruising and bleeding tendencies, swelling of the legs and accumulation of fluid in the peritoneal cavity (the area that separates the organs from the abdominal wall). Eventually, cirrhosis may lead to various complications such as esophageal varices (enlarged veins in the wall of the esophagus that can cause life-threatening bleeding) hepatic encephalopathy (confusion and coma) and hepatorenal syndrome (kidney dysfunction).
Hepatitis C
Much like hepatitis B, acutely infected individuals may clear the virus completely from their system and be hepatitis-free, and those who don’t become chronically infected. But the disease will become chronic in a much higher percentage of infected individuals – up to 90% can carry the disease indefinitely. 75% of these individuals will experience only mild to moderate liver damage over their lifetime. However, in approximately 25% of cases, chronic hepatitis can lead to serious problems such as liver cirrhosis, liver failure or liver cancer over a period of 25 to 30 years.
Individuals are more likely to develop cirrhosis if they drink alcohol, are obese, are male, became infected after age 40, have another type of liver disease or have another chronic infection (such as HIV or hepatitis B) in addition to hepatitis C.
Prevention/management: Vaccines are available for both hepatitis A and hepatitis B (available as separate vaccines or combined into a single vaccine), but not for hepatitis C. Because hepatitis is caused by a virus, antibiotics are ineffective against all three viruses.
Hepatitis A
There is no drug treatment for hepatitis A. The disease will eventually run its course and an infected person will recover completely, although recovery time varies for each person. Recovery from this viral infection means that the body has developed the antibodies necessary to prevent an individual from ever getting it again.
Effective preventive measures include:
- Washing your hands frequently and thoroughly especially after using the washroom, before preparing food and before eating
- Avoiding raw or undercooked food
- Since up to 40% of the reported cases of hepatitis A occur in travellers, it is advisable to protect yourself with a hepatitis A vaccination before you plan to travel, which when taken as two doses 6 months apart can protect you for up to 20 years
- If you will be travelling to a country with high rates of hepatitis A:
- Drink bottled or boiled water and use it for brushing your teeth
- Drink bottled beverages without ice
- Avoid uncooked food including salad
- Avoid food from street vendors
- Peel and wash fresh fruits and vegetables yourself
Hepatitis B
Aside from vaccination, the only known treatment for acute hepatitis B is an injection of hepatitis B immune globulin that may prevent development of the disease, provided exposure has been within 7 days.
Two types of treatment exist for chronic hepatitis B – interferon (synthetically manufactured human antiviral protein) injections and oral antiviral medications (i.e. lamivudine, adefovir, telbivudine, tenofovir, and entecavir). While these treatment do not cure, they help control the virus so that further liver damage can be prevented.
Because hepatitis B has no symptoms until the liver is badly damaged, a regimen of regular lifelong blood tests is the only method for determining whether hepatitis B is active or inactive, and whether treatment is needed.
Individuals who suffer from chronic hepatitis B can help minimize liver damage by keeping their body and immune system strong through avoiding alcohol, following a healthy, nutritious diet and exercising regularly.
Women who are pregnant and infected with hepatitis B should know their infant is at a high risk of becoming a chronic carrier. In Canada, it is recommended that infants born to infected mothers receive a special injection immediately after birth and a first dose of vaccine within 12 hours of birth to help prevent infection.
Hepatitis C
Drug treatment (pegylated interferon injections + ribavirin pills) may be effective for some hepatitis C infected individuals, with cure rates ranging from 40 to 90%, depending on the strain of hepatitis C involved. No alternative therapies which include herbal remedies, homeopathic medicines, and minerals have been proven safe and effective for treatment of hepatitis C.
The most commonly reported symptom of chronic hepatitis C is fatigue. Regular exercise and healthy eating can help a chronic hepatitis C individual feel more energized.
It is important to understand that people with a chronic hepatitis B or hepatitis C infection are at risk of transmitting the virus to others. Because time between initial contact and the onset of any symptoms ranges from two to six months and only about 50 percent of people ever develop symptoms, it is possible for people to spread the virus without even knowing they are infected.
Additional information: Canadian Liver Foundation, Health Canada, Wikipedia
|
 |
Definition: Cholesterol is a form of fat, or lipid, which exists within all our cells to help build/repair them. In addition, the body uses cholesterol to produce hormones, vitamin D, and substances which help digest foods. Your body makes all the cholesterol it needs, but we also consume it in our diet when we eat animal products and this is generally what causes total blood cholesterol level to increase past the safe limit of 5.2 mmol/L (200 mg/dL).
High blood cholesterol is a major risk factor for cardiovascular disease for women, particularly when combined with smoking and high blood pressure. According to the Canadian Heart Health Survey, 43% of Canadian women aged 18-74 have a total cholesterol level above the recommended threshold of 5.2 mmol/L. The percentage increases from 17% among women aged 18 to 24, to a high of 78% among women aged 55 and over (i.e. after menopause). While high cholesterol, or hypercholesterolemia, is not a disease, it does increase your odds of getting heart disease. There are no symptoms of high cholesterol, so there is no way of knowing whether you have it or not unless you are checked by a physician.
There are two types of cholesterol found within our bodies: HDL or high-density lipoproteins (healthy) cholesterol and LDL or low-density lipoproteins (lousy) cholesterol.
LDL cholesterol is the cholesterol that will build up as fatty deposits (plaque) inside blood vessels, which narrows the arteries (atherosclerosis) and contributes to coronary artery disease (CAD) and/or peripheral artery disease (PAD). If the fatty deposits break free from the arterial walls it could form a clot and travel in the blood back to the heart, causing angina or even a heart attack.
HDL cholesterol helps carry LDL cholesterol away from blood vessel walls. HDL cholesterol may also protect us from heart disease, so the higher the level of HDL to LDL the better. The ratio total cholesterol to HDL cholesterol is therefore a better indicator of cardiovascular risk than total cholesterol alone.
Here are the recommended target levels for cholesterol. However, blood cholesterol can be affected by a number of different things and so your physician is best qualified to determine what the ideal target rates should be for you.
- Total cholesterol less than 5.2 mmol/L (200 mg/dL)
- An LDL cholesterol less than 3.5 mmol/L. (about 130 mg/dL)
- An HDL cholesterol higher than 1.0 mmol/L for men and 1.2 mmol/L for women (about 40 mg/dL)
- A total cholesterol/HDL cholesterol ratio less than 5.0
Although not classified as cholesterol, another type of fat called triglycerides is often measured during a standard cholesterol test. Triglycerides can increase blood’s tendency to clot, increasing the risk of a heart attack or stroke, particularly if one also has high levels of LDL. It is generally recommended that total triglyceride level within the blood not exceed 2.2 mmol/L.
Known or suspected causes:
- Diet: Too much saturated fat and cholesterol can raise cholesterol. Saturated fat and cholesterol are found in animal products (i.e. beef, pork, veal, milk, eggs, butter, cheese), many packaged foods, stick margarine, sour cream, salad dressings, marinades, mayonnaise, shortening and snack foods like cookies, crackers and chips.
- Weight: Excessive weight can raise triglycerides and lower healthy HDL.
- Activity: Lack of exercise can raise lousy LDL and lower healthy HDL.
- Age: In women, cholesterol stays fairly low until menopause, before rising to equal and eventually surpass levels found in men.
- Genetics: There is an hereditary factor. In some cases, a rare disease can cause very high cholesterol with very low HDL and high triglycerides.
- Mental stress: This may be more related to our tendency to eat “comfort” foods when we’re stressed which are generally high in cholesterol.
- Diabetes: Diabetes can affect the balance of HDL and LDL cholesterol. (Note that diabetics tend to have stickier LDL particles because they are more coated with glucose which makes them tend to remain in the bloodstream longer and therefore have more chance to attach to the blood vessel walls. Also, diabetics tend to have low HDL and high triglyceride levels, which makes them more prone to heart disease.)
- Kidney disease: Nephrotic syndrome
- Hypothyroidism: High cholesterol is a less common symptom of hypothyroidism.
Consequences of High Cholesterol: There is a link between high cholesterol and heart disease, stroke, diabetes and other health problems.
- Coronary heart disease (main risk), caused by build up of plaque in the arteries near the heart, reducing blood flow to it. This can result in angina (chest pain) or heart attack.
- Stroke, caused by plaque build up blocking flow of blood to the brain.
- Peripheral Artery Disease, caused by plaque limiting flow of blood to rest of body.
- High blood pressure, caused by plaque restricting circulation so that the heart has to pump harder to circulate enough oxygen rich blood through the body.
Prevention/management: Lifestyle changes and medications, with the goal being to lower LDL and perhaps increase HDL. Lifestyle changes include reducing the amount of saturated fat within the diet and eating more soluble fibre*, losing weight (even 5-10 lbs can lower cholesterol and triglycerides), being more physically active and quitting smoking. When lifestyle changes are not enough, cholesterol lowering drugs called statins are usually prescribed, sometimes in combination with other drugs designed to lower triglycerides or raise HDL.
*Soluble fibre, found in foods such as oat bran, oatmeal, dried beans (legumes), beans, barley, apples and citrus fruit, has been shown to absorb dietary cholesterol and thus prevent it from entering the blood stream.
Additional information: Heart and Stroke Foundation of Canada, Quaker Cholesterol Challenge, Understanding Heart Disease, MSN Health & Fitness, Wikipedia
|
 |
Definition: Hyperlipidemia means having higher than normal levels of lipids in the blood. There are different types of blood lipids, but the most common are cholesterol and triglycerides. The term hypercholesterolemia is used when it is cholesterol specifically that is elevated, and similarly hypertriglyceridemia means high triglyceride levels. Note that "lipids" and "fats" tend to be used interchangeably, but in reality fats are but one subgroup of lipids.
Lipids travel through the bloodstream by attaching to protein molecules and forming lipoproteins. While there are several types of lipoproteins in the blood, LDL (low density lipoprotein) and HDL (high density lipoprotein) are the most commonly measured. Because both of these lipoproteins are used to carry cholesterol through the bloodstream, they are often referred to as LDL cholesterol and HDL cholesterol.
Known or suspected causes: Hyperlipidemia is quite prevalent in the North American population, in large part due to diet and lifestyle. The following factors have been identified as possible causes of hyperlipidemia:
- Alcohol abuse - Alcohol spurs the liver to make more triglycerides, and even light drinking (two to four ounces of wine a week) can raise triglycerides. (Diabetes Organization, Feb. 2000, and Tufts University Health & Nutrition Letter, July 1997). In addition, alcohol is a major source of excess calories which get turned into fat, so the triglyceride levels in the blood increase. Alcohol also has been shown to inhibit the burning of fat. A 2003 study conducted in Geneva, Switzerland found that alcohol in the bloodstream can slow down fat metabolism by more than 30%. (Journal of the American Medical Association. July 2003).
- Cholestasis - Cholestasis is caused by an obstruction within the liver (widespread blockage of small ducts, disorders such as hepatitis) or outside the liver (tumors, gallstones, side effect of medications, complications of surgery, pregnancy, oral contraceptives) which causes triglycerides (and also bile salts and bilirubin) to accumulate in the blood stream instead of being eliminated normally.
- Chronic renal failure or kidney disease - Several studies have found a relationship between impaired kidney function and elevated triglycerides in the blood.
- Diabetes mellitus - Insulin resistance causes fat cells to release fatty acids into the bloodstream.
- Glycogen storage diseases - When your body lacks an enzyme required to break down a specific type of sugar (i.e. sucrose, lactose, etc.), hypoglycemia (low blood sugar) will result. Triglycerides and other by-products of metabolism increase in the blood as the body tries to raise blood sugar.
- Hypothyroidism - Commonly causes LDL (low density lipoprotein) elevations but also may lead to mixed hyperlipidemia or isolated triglyceride elevations.
- Certain medications - Diuretics and beta-blockers have been known to increase blood serum lipids. Glucocorticoids raise HDL and may also increase triglycerides and LDL. Retinoids increase triglycerides and LDL and also reduce HDL. Interferons can cause hypertriglyceridemia. Hormonal replacement therapy may cause massive hypertriglycerademia in susceptible women - one study reported an 18 year old woman whose triglyceride levels went from 3.95 mmol/L to 58.78 mmol/L.
- Obesity - The relationship between obesity and elevated triglyceride levels has been clearly established through a number of studies.
- Oral contraceptives - Studies have shown that oral contraceptives (birth control) increase both triglycerides and total cholesterol.
- Pancreatitis - The pancreas releases digestive enzymes into the small intestine to digest carbohydrates, proteins and fat. When the pancreas becomes inflamed or infected, it cannot function properly and release the digestive enzymes. This causes a build-up of fats in the bloodstream and creates high levels of triglycerides. Ironically, high levels of triglycerides can cause pancreatitis, creating an ongoing vicious cycle that causes both the pancreatitis and the hypertriglyceridemia to worsen.
- Positive family history - Familial combined hyperlipidemia, a disorder of high cholesterol and high blood triglycerides, is caused by a genetic defect that is passed from parent to child. People with this disorder tend to develop high cholesterol or triglyceride levels during their teenage years, with levels remaining high throughout life. People with familial combined hyperlipidemia have an increased risk of early coronary artery disease and heart attack, and typically have higher rates of obesity and glucose intolerance. Familial hypertriglyceridemia also exists, where triglyceride levels are high but cholesterol remains relatively normal.
- Pregnancy - Triglyceride levels normally increase during the last trimester of pregnancy, so that hyperlipidemia in pregnant women can be serious and even life threatening when associated with severe hypertriglyceridemia and pancreatitis.
- Hypolipoproteinemia - Hyperlipoproteinemia is a metabolic disorder characterized by abnormally elevated concentrations of specific lipoprotein particles in the plasma. By the very nature of this disorder, in all cases of hyperlipoproteinemia, hyperlipidemia is present.
- Progeria short stature pigmented nevi - Though not present in all cases of this very rare inherited disorder characterized by premature aging, short stature, and immune system deficiency, hyperlipidemia is a possible symptom.
- Sedentary lifestyle - Physical inactivity can lead to weight gain, which increases one's risk for hyperlipidemia. Conversely, physical exercise has been shown to raise HDL and lower LDL and thus help keep cholesterol and triglycerides in line.
- Smoking - Studies have shown that the concentration of high-density lipoprotein (HDL) cholesterol (the "healthy" cholesterol) is lower in heavy smokers, and concentrations of triglycerides and cholesterol are higher.
Consequences of Hyperlipidemia: Although lipids, and specifically fats, have been given a bad rap, they are in fact essential for our survival. Not only are lipids necessary for adequate energy storage, they also hold our cells together, transport enzymes and nutrients into our cells and prevent foreign bodies from entering and doing damage. In addition, lipids are also involved in the production of hormones and vitamins.
However, moderation is the key, since excessive lipid levels in one’s bloodstream can lead to significant health problems. High cholesterol levels, in particular, lead to atherosclerosis, or hardening of the arteries. Cholesterol is sticky, and when too much of it is in the blood (transported via LDL – low density lipoprotein) it starts to adhere to blood vessel walls in the form of arterial plaque that could eventually build up to such an extent that blood flow is significantly reduced. Depending on where the build up occurs, this could lead to heart attack or stroke. Click here for a short video that describes how this process works.
Studies have shown that high triglyceride levels are linked to increased risk of heart disease and stroke, although not all scientists agree that triglycerides and heart disease are directly correlated. It is quite possible the correlation is due to the fact that people with high triglycerides tend to have high levels of LDL cholesterol along with low levels of HDL cholesterol – two factors which are definitely linked to heart disease. There is growing acceptance that the best predictor of heart disease is a triglycerides/HDL ratio, and that for this ratio anything under 2 is generally "safe". Note that as your triglyceride level increases or your HDL (good lipoprotein cholesterol) decreases, the ratio goes up.
According to healingdaily.com, people with triglyceride levels greater than 200 mg/dl (2.3 mmol/L) are 30% more likely to have an ischemic stroke than people with more normal levels (less than 150 mg/dl or 1.7 mmol/L). In addition, a high level of blood triglycerides (greater than 500 mg/dL or 5.6mmol/L) increases your risk of fatty liver disease and acute
pancreatitis.
Prevention/management: The main goal of treatment is to reduce the risk of atherosclerotic heart disease specifically and coronary heart disease in general.
In order to bring your levels of cholesterol and/or triglycerides under control, any potential underlying medical problems (i.e. diabetes, hypothydroidism) need to be identified and treated. In addition, lifestyle changes such as dietary adjustments, weight reduction and exercise will be required. If that is not sufficient, then drug therapy may be suggested by your doctor.
Your doctor’s recommended dietary changes may include:
- Reducing saturated fat intake as well as total fat intake.
- Limiting dietary cholesterol by reducing the amount of animal protein consumed, particularly egg yolks and organ meats.
- Eating a more vegetarian diet (cholesterol exists only in foods of animal origin, and animal-based foods are also the primary source of saturated fat in your diet).
- Eating more soluble fibre, found in foods such as oats, barley, peas, beans, and certain fruits and vegetables.
- Eating more cold water fish (mackerel, sardines, salmon), which contain omega-3 fatty acids (omega-3 fatty acids are known to lower triglycerides).
- Eating more unrefined, low-glycemic-index carbohydrate sources, such as legumes and most whole grains.
- Using all fats and oils sparingly, if at all. Consuming small amounts of fats in their naturally occurring form (eg, nuts) may be preferable to using oils because of their potentially cardioprotective nutrients: magnesium, fiber, vitamin E, and flavonoids.
- Avoiding alcohol, which increases blood triglyceride levels.
Worthy of note:
- Soybeans found in tofu, soy nuts and many meat substitutes contain a powerful antioxidant that can lower LDL.
- Psyllium, a soluble fibre made from seed grain husks, helps absorb water and cholesterol from your intestines and may improve the ratio of HDL to LDL.
- Nuts (almonds, peanuts, pecans, and walnuts) appear to have lipid-lowering effects, apparently due to their fiber, plant sterol, and unsaturated fat content.
- Plant sterols (often in the form of margarine) reduce LDL cholesterol concentrations by roughly 10% by inhibiting cholesterol absorption.
- The combination of a vegetarian diet, soluble fiber, soy protein, nuts, and plant sterols has been shown to lower LDL by nearly 30% in short-term clinical trials, an effect similar to that of statins. Although each of these foods alone contributes to lowering lipids, their effects are complementary when the foods are combined.
- While a low fat diet will help lower triglycerides, a high sugar diet will increase them! Recent evidence indicates that the most important dietary precursor of triglycerides appears to be carbohydrates - sugars, starches and refined grains. Carbohydrates require insulin secretion, which is a potent stimulus to the liver to produce triglycerides.
Weight loss will help increase HDL cholesterol and lower both LDL cholesterol and triglyceride levels, particularly if you incorporate exercise into your daily routine. Your total weight loss goal will be determined in part by your body shape – people who carry their excess weight around their tummy area are at greater risk for heart disease than individuals whose weight is spread over their hips, thighs and bottoms, so if you fall into the higher risk category greater weight loss will be required to bring you into the “safe” zone.
Quitting smoking is imperative, since smoking can lower HDL, narrow your blood vessels, and injure your blood vessel walls, all of which will speed up atherosclerosis, or hardening of the arteries.
If you are taking oral contraceptives you may need to consider an alternate method of birth control, since they increase both cholesterol and triglyceride levels.
If diet and exercise are not enough to bring your hyperlipidosis under control, then you may require lipid-lowering medications such as:
- Statin drugs, which prevent your liver from manufacturing cholesterol.
- Bile acid sequestrants, which prevent your body from reabsorbing the cholesterol in bile. (Bile is a liquid secreted into your small intestine that helps you digest dietary fats.)
- Fibrates, which lower triglycerides and LDL as well as raise HDL.
- Niacin (vitamin B5), which in nicotinic acid form, can help lower LDL cholesterol and raise HDL cholesterol. However, it must be taken in therapeutic doses to be effective. (There are some serious side effects associated with large dosages of Niacin, so do not attempt to self medicate.)
Additional information: HealthScout.com MedlinePlus Up To Date for Patients University of California, San Diego Medical Center VascularWeb.org NutritionMD.org University of Minnesota School of Public Health U.S. Department of Health and Human Services National Cholesterol Education Program HighTriglycerides.com Cleveland Clinic
|
 |
Definition: Blood pressure is the force exerted on the arteries as the heart pumps blood throughout the body. There are two measurements associated with a blood pressure reading – the higher number (systolic pressure) measures the pressure created as the heart pumps and the lower number (diastolic pressure) indicates the pressure as the heart rests and refills between beats.
Blood pressure is constantly changing as we move around, but for an adult it should normally remain below 120/80 mm Hg (millimeters of mercury).
- Normal range: less than 120/80
- Prehypertension: 120-139/80-89 (Warning zone; high risk of developing hypertension)
- Stage 1 Hypertension: 140-159/90-99
- Stage 2 Hypertension: 160+/100+
- Hypertensive crisis: 180/110 + (Considered a life threatening medical emergency)
Note that in people with diabetes or kidney disease, blood pressure of 130/80 is considered high and should be treated.
According to recent estimates, 1 in 3 adults in the US have high blood pressure, but because there are no symptoms about 1/3 of these people don’t even know it. That being said, extremely high blood pressure can cause symptoms such as severe headache, fatigue or confusion, vision problems, chest pain, difficulty breathing, irregular heartbeat and blood in the urine.
Generally speaking, the lower the blood pressure, the better. However, severely low blood pressure can indicate serious heart, endocrine or neurological disorders and can deprive the brain and other vital organs of oxygen and nutrients, leading to shock, which can be a life-threatening condition. There is no specific number at which blood pressure is considered too low. However, a sudden fall in blood pressure can be dangerous — even a change of just 20 mm Hg can cause dizziness or fainting. Some rapid falls in blood pressure indicate a deeper underlying problem such as uncontrolled bleeding, severe infections or allergic reaction.
Known or suspected causes: For the vast majority of cases, the exact cause is unknown and this is called essential or primary hypertension. In secondary hypertension, the direct cause can be linked to a specific health issue such as kidney abnormality, birth defect such as structural abnormality of the aorta (large blood vessel leaving the heart) or narrowing of certain arteries. With secondary hypertension, the cause can usually be corrected, generally through surgery.
Controllable risk factors include: smoking, overweight or obesity, high salt intake, excessive alcohol consumption, physical inactivity, stress, chronic kidney disease and adrenal and thyroid disorders.
Women who are pregnant or taking birth control pills are also at higher risk of developing hypertension.
Uncontrollable risk factors include: family history, race (black people are more prone to high blood pressure than white people and tend to develop it earlier in life), and age (women are at a higher risk after menopause).
For younger people, diastolic pressure (the second number that measures pressure when the heart is refilling) is the main measure used to diagnose high blood pressure and risk of cardiovascular disease. The systolic pressure (first number that measures the pressure when the heat beats) is considered the more important number in middle aged and older adults. As we age our arteries tend to stiffen, which causes an increase in systolic pressure. Diastolic pressure, on the other hand, rises to about age 50 and then levels off and may eventually drop as we move into our more senior years.
Consequences of Hypertension: Stroke, heart attack, heart failure, kidney failure or vision problems.
Healthy arteries are muscular and elastic so that they stretch as the heart pumps blood through them. High blood pressure contributes to hardening of the arteries (atherosclerosis).
As arteries lose their elasticity, blood pressure increases, the heart becomes strained and blood vessels can become damaged so that the organs they are supplying, such as the brain or kidneys, become damaged as well. The brain, heart and kidneys can handle the increased pressure for a long time, which is why people can have high blood pressure for years with out knowing it. But that doesn’t mean damage isn’t occurring and sooner or later the organs will become damaged enough to stop functioning properly.
Prevention/management: Lifestyle modification, with medication in more severe cases. Lifestyle modifications such as losing weight, dietary changes, salt reduction, quitting smoking, reducing alcohol intake and increasing physical activity are not optional – no medication is available to offset the damaging effects of continued unhealthy living.
Managing high blood pressure is a life long commitment as there is no cure.
Because there are usually no symptoms associated with high blood pressure, if you are over 35 you should have your blood pressure checked at least once per year.
Additional information: Canadian Heart and Stroke Foundation, American Heart Association, WebMD, Wikipedia
|
 |
Definition: A group of inflammatory conditions of the large and small intestines, with the most common being Crohn’s disease and ulcerative colitis. Although very different diseases, they share similar symptoms so that it is sometimes difficult to identify which disease is present.
But while Crohn’s disease can affect any part of the gastrointestinal tract, ulcerative colitis occurs only in the colon (large intestine). And while Crohn’s affects the entire intestinal wall in patches, ulcerative colitis affects only the superficial layers of the large intestine (mucosa) in a more even and continuous distribution. Ulcerative colitis can be “cured” by surgically removing the affected area, but Crohn’s disease will almost always recur after surgical removal of diseased tissue.
Known or suspected causes: The exact cause of inflammatory bowel disease (IBD) has not been identified to date, although family history, race and ethnicity are suspected to play key roles in the development of the disease. 10-20% of individuals with IBD have a family history of the disease and family history is thus the greatest risk factor for IBD, particularly when the family member is a first degree relative. While IBD can occur at any age, it is most commonly diagnosed between 15-35 years of age, with men and women equally affected.
The highest rates of IBD occur among Caucasians, particularly those of Jewish descent, whose risk is 3-6 times greater.
In addition to genetic factors, it is thought that environmental factors (such as infections) which compromise the immune system may contribute to the development of the disease in predisposed individuals.
Scientists have recently identified the first gene specifically linked to Crohn’s disease and ongoing research is looking into how defects in this gene might lead to the disease, as well as what other genes might be related to IBD.
Consequences of Inflammatory Bowel Disease: The most common symptom of IBD is diarrhea, brought on by an accumulation of white blood cells in the lining of the intestines that causes inflammation. The nature and degree of additional symptoms depends on the severity and duration of the inflammation, and can include ulcers, bleeding, strictures (scarring that causes narrowing of the intestinal wall and bacteria overgrowth of the small intestine) and fistulas (tubular passageways originating from the bowel wall and connecting to other organs or the skin). The more widespread the inflammation of the small intestine, the higher the risk of malnutrition due to malabsorption of nutrients. Chronic inflammation may also lead to colon cancer, and individuals with IBD have a risk of colon cancer twenty times higher than that of the normal population.
Complications outside the intestines can also develop, including arthritis, skin rashes, eye problems and liver disease. Refer to the individual write ups for Crohn’s disease and ulcerative colitis for more specific details.
Most individuals are able to lead relatively normal, productive lives, although may need to be occasionally hospitalized during acute flare ups. Medication will be required in most cases to keep inflammation and its related complications under control.
Prevention/management: Drugs, nutrition supplements and sometimes surgery are utilized to control inflammation, correct nutritional deficiencies and relieve symptoms like abdominal pain, diarrhea and rectal bleeding. In severe cases, a portion of the colon and sometimes even the entire colon will need to be removed through a colectomy and a pouch worn to collect waste product that no longer can exit normally through the anus.
Additional information: Crohn's & Colitis Foundation of Canada, Wikipedia, Medicine Net, Healthline
|
 |
Definition: A chronic disorder of the bowel (specifically the colon or large intestine) producing cramping, abdominal pain, bloating, constipation and diarrhea. Though it causes a great deal of discomfort, unlike inflammatory bowel disease (including Crohn’s disease and ulcerative colitis) it does not permanently harm the intestines nor does it lead to other health problems or diseases such as cancer. (However, some research sources such as Wikipedia and the Canadian Society of Intestinal Research report that people with IBS more commonly experience gastroesophageal reflux, sleep disturbance, fibromyalgia, headache and backache.)
IBS is classified as a "functional disorder" with altered patterns of intestinal muscle contractions rather than a "disease".
IBS is estimated to affect 13-20% of Canadians, and in some countries estimates run as high as 30% of the population, making it the most common gastrointestinal diagnosis worldwide. In Canada (and most Western nations), IBS occurs more often in women than men, but in some countries such as India it’s the other way around. Although IBS can occur at any age, it begins before the age of 35 in about 50% of all cases.
When the colon does not contract properly, the contents inside the colon do not move correctly, which is what creates the pain, discomfort and either constipation (contents move too slowly so too much water is absorbed by the colon) or diarrhea (contents move too quickly so not enough water is absorbed).
Known or suspected causes: The specific cause of IBS is not yet known, although scientists suspect that people who suffer from IBS have a colon (large intestine) that is highly sensitive and reactive to certain foods and stress.
In some cases bacterial infection appears to be the trigger and incidences of IBS arising from infection have been termed "post-infectious IBS".
There is also some evidence to indicate that IBS is affected by the immune system and/or may be the result of an as yet undiscovered active infection.
Consequences of Irritable Bowel Syndrome: Symptoms vary from person to person, but the main symptoms of IBS include pain, bloating and discomfort. Most people can control their symptoms through diet, stress management and medication, but for some the disorder can be disabling enough that they can’t work, attend social events or even travel for short distances. Clearly this can seriously compromise quality of life.
For some IBS causes constipation and for others it leads to diarrhea, and some people experience both. The diarrhea can create a frequent and uncontrollable need to have a bowel movement, so that quick access to washroom facilities at all times is mandatory. Sometimes symptoms subside for a few months before returning, and in other cases symptoms constantly worsen over time.
Additional symptoms can include whitish mucus in the stool, a swollen or bloated abdomen and the feeling that a bowel movement is not yet finished. Women often have exacerbated symptoms during their menstrual period.
The consequences of IBS can cause a person to feel depressed and anxious, which in turn can further worsen symptoms since stress can stimulate colon spasms in people with IBS. (Kind of like the “butterfly” sensation normal people get when they’re nervous, but with much more drastic consequences.) Loss of self esteem, shame, fear, self-blame, guilt or anger may also be experienced, which can be quite damaging to one’s sense of well being.
Unfortunately, only about 10% of individuals with IBS symptoms seek the help of a physician, so the vast majority of sufferers do not get the help they need to control symptoms and make the disorder more manageable for day-to-day life.
Bleeding, fever, weight loss and persistent severe pain are not symptoms of IBS and may be indicative of inflammation or in rare cases, cancer.
Prevention/management: There is no specific test for IBS, which is generally diagnosed once other disorders have been ruled out. Stool samples, blood tests, x-rays and colonoscopy may be used in conjunction with a careful analysis of reported symptoms to make the final diagnosis.
There is no cure for IBS, but there are several options available to manage symptoms. Fiber supplements or laxatives can help with constipation and medications such as Imodium can help reduce diarrhea. Anti-spasmodic drugs can help control colon muscle spasms and thereby reduce abdominal pain (but can also contribute to constipation). Prescription medication is available in more severe cases, but should be used with caution as side effects can be significant.
Although each individual is different, the following are known to worsen symptoms in many cases: eating large meals as opposed to smaller, more frequent ones, ingesting certain medicines, wheat, rye, barley, chocolate, MSG, milk products, fatty foods, alcohol, drinks with caffeine (coffee, tea, colas) or carbonated beverages and experiencing stress, conflict or emotional upset. (While stress does not cause IBS, it can worsen symptoms.)
Drinking six to eight glasses of water a day is important, particularly if diarrhea is present. High fibre foods will help with constipation by creating looser stools and also with diarrhea by absorbing excess water. Diets higher in carbohydrates than fats have been known to help. Chewing gum and eating too quickly can lead to swallowing air, which will in turn lead to gas.
Adequate sleep and physical exercise have been shown to have a positive effect on symptoms.
Additional information: Canadian Society of Intestinal Research, Irritable Bowel Syndrome Association, Wikipedia, National Digestive Diseases Information Clearinghouse
|
 |
Definition: Kidney disease (sometimes referred to as chronic kidney disease or CKD) is a general term which refers to the gradual and usually permanent loss of kidney function over time. CKD is diagnosed once kidney damage or impaired kidney function has been present for a minimum of three months, and it is measured using five stages of severity:
| Stage 1: |
Slight kidney damage with normal or increased filtration |
| Stage 2: |
Mild decrease in kidney function |
| Stage 3: |
Moderate decrease in kidney function |
| Stage 4: |
Severe decrease in kidney function |
| Stage 5: |
Kidney failure (kidney is working at less than 10% of full capacity) requiring dialysis or transplant |
Tiny filters (nephrons) inside the kidneys perform 3 main functions – removal of wastes from the blood, regulation of water and various mineral levels within the body and production of hormones which control other body functions, such as bone maintenance, production of red blood cells and regulation of blood volume and blood pressure. Kidney disease damages the nephrons, so that their ability to do their job becomes compromised.
Chronic kidney disease tends to start slowly and progress over a number of years. Caught in the early stages, the damage can often be slowed down or stopped; however, left unchecked kidney disease will ultimately lead to total kidney failure. But because there are almost no symptoms until over 50% of the nephrons have been damaged, kidney disease is often not diagnosed until it is quite advanced.
Initial symptoms which may trigger your health care provider to check for kidney disease include:
- High blood sugar - when diabetes is not under control
- Hypertension - when blood pressure is not under control
- Fatigue
- Loss of appetite
- Headaches
- Generalised and persistent itchy skin
- Changes in urination - making more or less urine than usual, feeling pressure when urinating, changes in the color of urine, foamy or bubbly urine, or having to get up at night to urinate
Symptoms which appear in the later stages of the disease once toxins begin to accumulate in one’s blood may include:
- Hematuria (blood in the urine), eventually leading to anemia
- Trouble concentrating or dizziness (due to accumulation of waste products)
- Puffy eyes, hands, legs and feet (due to fluid retention)
- Numbness in the feet or hands (caused by nerve damage)
- Abnormal levels of potassium, calcium and/or phosphate (kidneys are no longer able to filter these minerals from the body)
- Acidosis (excessive acidity of body fluids)
- Bone disease - pain and fractures (due to impaired bone maintenance hormone production)
- Back or flank pain (the kidneys are located on either side of the spine in the back)
- Chest pain (due to pericarditis - inflammation around the heart)
- Shortness of breath (due to fluid in the lungs)
- Feeling cold
- Nausea and vomiting
- Thirst
- Bad taste in the mouth or bad breath
- Weight loss
- Excess bleeding (due to poor clotting)
- Muscle twitching or cramping, including restless leg syndrome
- Yellowish-brown tint to the skin
- Decreased sexual interest and erectile dysfunction
- If diabetic, more hypoglycemic episodes
Chronic kidney disease can result from a variety of different causes, and symptoms will vary depending on the type of kidney disease a person has. For example, if the cause is bacterial infection, high fever will result. Polycystic kidney disease (PKD), a relatively common cause of kidney failure in North America, is a genetic condition which causes cysts to develop throughout the kidneys. Cysts vary in size and number and may eventually cause kidney damage if they become large and numerous. The most common symptoms of PKD include back or side pain, or a feeling of fullness.
Other symptoms of PKD include:
- Kidney infections (quite common)
- Liver and pancreatic cysts
- Kidney stones (occurs in 20% of cases)
- Hypertension (high blood pressure – occurs in 60-70% of cases and may be the first sign of the disease)
- Abdominal pain (from the enlarged kidneys pressing on the abdomen)
- Puffy eyes, hands, and feet (called edema)
- Increased urination, especially at night
- Bloody urine
- Pain or difficulty passing urine
- Varicose veins
- Hemorrhoids
- Headaches
Chronic kidney disease should not be confused with acute kidney failure. Unlike chronic kidney disease which progresses slowly over time, acute kidney failure develops rapidly over days or weeks as a result of something that is directly affecting the kidney, its blood supply or urine flow from it. Acute kidney failure does not usually cause permanent damage to the kidneys, and with appropriate treatment it is often fully reversible. In some cases, however, acute kidney failure may progress to chronic kidney disease.
Chronic kidney disease is a significant and growing health problem in the United States and Canada. The Kidney Foundation of Canada estimates as many as 2 million Canadians have kidney disease, although many may not be aware of it. The Center for Disease Control (CDC) in the US reports that approximately 26 million Americans have chronic kidney disease and another 20 million are at risk, and that 85,000 Americans die each year from kidney failure.
It’s believed the increasing incidence of kidney disease is related to the higher levels of diabetes, high blood pressure and obesity within the North American population. Chronic kidney disease is most common among Hispanic, African/Caribbean, Asian or Pacific Islander, and Native American people, and approximately 40% of people with kidney disease are 60 years or older.
Known or suspected causes: Complications from diabetes is the leading cause of chronic kidney disease (responsible for about 40% of all kidney failure); when blood glucose remains high over an extended period, the kidney’s blood vessels and filters (nephrons) are damaged. Therefore, if you have diabetes, it is critical to keep your blood glucose levels as close to normal as possible.
High blood pressure is the second leading cause of chronic kidney disease (about 25% of all kidney failure). Much like high blood glucose levels, high blood pressure also damages blood vessels and filters within the kidneys so that kidney function is impaired.
Other causes of chronic kidney disease include:
- Kidney infection (bacterial, viral or parasitic) and/or repeated urinary infections
- Glomerulonephritis, a group of diseases which cause inflammation and damage to the filtration system and may themselves be caused by post-infectious conditions or lupus
- Atherosclerosis (hardening of the arteries, which damages the blood cells in the kidneys)
- Trauma or injury to the kidneys
- Kidney stones which obstruct the flow of urine
- Enlarged prostate (can block the system which drains the kidneys)
- Autoimmune diseases such as Lupus
- Certain prescription or street drugs
- Prolonged use of certain non-prescription pain killers such as NSAIDs (ASA-Aspirin, Ibuprofin-Motrin, Advil) or acetaminophen (Tylenol)
- Certain poisons
- Inherited diseases such as polycystic kidney disease
- HIV infection
- Sickle cell disease (genetic blood disorder)
- Heroin abuse
- Amyloidoisis (abnormal protein deposits)
- Certain cancers
Risk factors include:
- Diabetes – danger of elevated blood glucose levels damaging blood vessels and filtration system
- Hypertension – danger of elevated blood pressure damaging blood vessels and filtration system
- Cardiovascular disease - heart attacks or strokes, congestive heart failure, coronary artery disease or peripheral vascular disease can all lead to kidney problems
- Liver disease
- Genetic & autoimmune diseases – amyloidosis, sickle cell disease, lupus
- Fibromuscular dysplasia – a disease which can cause hardening of the arteries within the kidneys
- Vasculitis or arteritis – a group of disorders that cause inflammatory destruction of blood vessels and arteries respectively
- Use of anti-inflammatory medications
- Vesicoureteral reflux (urine travels the wrong way within the urinary tract)
- Family history - People with a mother, father, brother or sister who has had kidney disease are more likely to develop kidney problems
- Age – people over 60 are at higher risk
- Race - certain ethnic groups, such as Hispanic, African/Caribbean, Asian or Pacific Islander and Native American people, are at a higher risk
Consequences of Kidney Disease: Kidney disease is a serious problem, with serious consequences. Because symptoms do not typically appear until the disease is quite advanced, a significant amount of damage can be done to the body before kidney disease is detected and corrective measures are taken.
As the disease progresses and the kidneys slowly become less efficient, toxins begin to build in the body which can lead to electrolyte imbalances that impair muscle coordination, heart function, fluid absorption/excretion, nerve function and concentration. This can also lead to acidosis (too much acidity in the blood), which breaks down proteins and causes inflammation and bone disease.
Fluid imbalances can lead to congestive heart failure and pulmonary edema (accumulation of fluid in the lungs). A build up of toxic waste in the body (called uremia) will cause fatigue, loss of appetite and excess fluid retention. In later stages uremia will lead to impaired mental functioning, seizures, coma and ultimately death.
Because the kidneys are involved with the production of red blood cells, reduced kidney function will eventually lead to anemia, which reduces the amount of oxygen in the blood and causes headaches, irritability or difficulty concentrating, along with reduced energy levels and impaired cell building/repair function.
The kidneys also produce hormones which regulate bone maintenance, and so bone disease is another possible complication of kidney disease.
Chronic kidney disease can eventually lead to total kidney failure, so that either kidney replacement or ongoing dialysis is required. In general, only 32% of dialysis patients survive past five years, and older people or those with diabetes fare much worse. The two year survival rate for kidney transplant patients when the donor is a living relative is 90%, and 88% when the donor was deceased.
With Polycystic kidney disease, there is a 5-10% chance of developing a brain aneurysm. Should the aneurysm rupture, symptoms will include sudden severe headache, nausea, vomiting and pain moving the neck, and immediate medical attention is required. With PKD, cysts may also appear in other parts of the body, including liver, pancreas, colon, testes and brain. Approximately 25% of people with PDK also develop weakened heart valves, sometimes to the point where valve replacement surgery is required.
Prevention/management: Chronic kidney disease cannot be prevented in most situations, but it may be possible to protect the kidneys from damage or slow the progression of the disease by controlling underlying conditions. Diabetes and hypertension need to be treated aggressively and kept under strict control so that potential for kidney damage is minimized.
Kidney disease is usually advanced by the time symptoms appear and therefore diabetics and others at high risk for developing chronic kidney disease should be screened regularly for it.
It is always a good idea to avoid exposure to drugs, chemicals and other toxic substances as much as possible, and street drugs, NSAIDs (nonsteroidal anti-inflamatory drugs, such as aspirin or ibuprofen) and Acetaminophen (Tylenol and Excedrin) in particular. Taking NSAIDs and Acetaminophen at the same time is particularly dangerous, even to people without compromised kidney function.
Ulcer medications (Tagmet, Zantac) could prove problematic, as well as Alka Seltzer (contains a lot of salt). Decongestants like pseudoephedrine (Sudafed) are cause for concern, especially for individuals with high blood pressure. Laxatives and antacids containing magnesium and aluminum should also be avoided. Some herbal medications will contain substances that are dangerous for individuals with compromised kidney function, so any herbal medication should be reviewed with a health care professional prior to taking it.
Quitting smoking and losing excess weight through a healthy diet and exercise plan will also alleviate the amount of stress placed on one’s kidneys, which will help slow the disease process. Certain dietary restrictions can delay the progression of chronic kidney disease:
- Protein – a certain minimum level is required to build, maintain and repair body tissues, as well as fight infections and heal wounds. However, protein produces urea, which can cause tiredness, nausea, headaches and a bad taste in the mouth if the kidneys are unable to efficiently filter it from the blood.
- Salt – reducing salt will help avoid fluid retention and high blood pressure. Processed foods like deli meats, canned foods, convenience and fast foods, salty snacks and salty seasonings all contain excess salt. Unsalted spices, herbs, vinegar and lemon can be used to flavour foods instead.
- Fluid – reducing fluid intake will place less strain on the kidneys and reduce the level of swelling in the body as less and less urine is able to be produced. Too much fluid can also cause high blood pressure and shortness of breath.
- Potassium – in advanced stages of kidney disease, the kidney are unable to remove potassium, which can cause abnormal heart rhythms. Foods high in potassium include bananas, oranges, nuts, squash, tomatoes, potatoes, dried peas and beans.
- Phosphorous – reducing phosphorous intake will slow down bone loss and alleviate both itchy skin and painful joints. Foods high in phosphorous include eggs, beans, seeds, nuts, dried peas, processed bran cereals, cola drinks and dairy products.
Pain from cysts produced in polycystic kidney disease can sometimes be managed by draining the cysts, which relieves pressure on the areas around them. In severe cases, the cysts may need to be removed via surgery, but this is usually only a temporary solution. Pain medication further stresses the kidneys so those taking it should be closely monitored by their health care provider.
There is no cure for either chronic kidney disease or polycystic kidney disease and so the goal of treatment is to keep the kidneys functioning as long as possible, until dialysis or transplant become the only viable survival options.
Few initial symptoms means that laboratory tests are required to properly diagnose the disease, which will be confirmed once an abnormal reading has been detected for a minimum of 3 months. Glomerular filtration rate (GFR) measures the rate at which the kidneys filter blood and is considered the best overall measure of kidney function. Other kidney disease indicators include high blood levels of creatinine and urea nitrogen or high levels of protein in the urine. Any urine test for kidney disease should include a measurement of microalbumin (small amounts of protein that don't show up on a standard urine test). The presence of white or red blood cells in the urine may be a sign of kidney infection or other forms of kidney disease.
Should blood or urine tests indicate a potential problem, a kidney x-ray or ultrasound can be used to identify polycystic kidney disease, cancer, kidney stones or other obstructions.
Should a problem with the kidneys be detected, treatment will depend on the original cause. Bacterial infections can be treated with antibiotics. Inflammation due to an immune reaction will be treated with immunosuppressant medications such as corticosteroids, but these will be effective on only some types of inflammation. If the problem is related to complications from diabetes, more strict control of blood glucose levels will be required. People with hypertension will need to bring their blood pressure to within acceptable limits to minimize any further kidney damage. A diuretic that forces the body to excrete more water and salt can help control the swelling associated with kidney disease, as can the voluntary limitation of salt and protein in the diet. Treating the underlying cause of acute kidney failure will often bring kidney function back to normal.
For end stage kidney failure, dialysis can either be done in a hospital or community setting (hemodialysis – filters toxins directly from the blood) or at home (hemodialysis or peritoneal dialysis – cleaning solution absorbs toxins from the abdominal lining). Kidney transplants have an 80% success rate, although powerful immune suppressants are required to prevent the body from rejecting the organ. Immune suppressants make the patient more susceptible to infections and some types of cancer, but it is generally accepted that the benefits of having a functioning kidney outweigh these risks.
Additional information: The Kidney Foundation of Canada, BC Government Ministry of Health Services, Healthy Ontario, Wikipedia, Canoe Health, Body & Health Canada
|
 |
Definition: A form of arthritis, and an autoimmune disorder where the body’s immune system produces antibodies which attack components of the cell nucleus and in some cases double stranded DNA. This disease affects nearly every organ system in the body, including the skin, joints, kidneys, heart, lungs, and central nervous system.
Symptoms include rash, photosensitivity, oral ulcers, arthritis, pleuricy, pericarditis, kidney problems, blood cell abnormalities, seizures and psychosis.
Neonatal lupus can occur when a mother with lupus passes auto antibodies to her child. Skin, liver and blood problems generally resolve by six months, but the most serious manifestation, congenital heart block, requires a pacemaker and has a mortality rate of about 20%.
Discoid lupus is a skin disorder that causes a red, raised rash on the face and scalp and occasionally (1–5%) develops into full blown lupus SLE.
Drug induced lupus is a temporary form of lupus caused by chronic use of certain drugs.
Lupus primarily affects women (6-10:1) and Blacks (and possibly Hispanics, Asians and Native Americans) more than Whites, but can occur from infancy to old age with most occurrences happening between ages 15-40.
Known or suspected causes: With the exception of drug induced lupus, the cause of this disease is unknown. While there is some evidence of hereditary factors, lupus is relatively uncommon. Current thinking is that a combination of genetic and environmental factors are responsible for the development of lupus.
Consequences of Lupus: There are many different symptoms associated with lupus because every organ system is affected and each system can be affected in different ways. But nearly everyone with lupus experiences severe fatigue which can be quite debilitating. Joint pain, another key symptom, is often what prompts the first doctor’s visit. People with lupus are at higher risk of various infections due to their compromised immune system.
In addition, other problems associated with lupus can include fatigue, fever, loss of appetite, weight loss, hair loss, muscle pain and weakness, headaches, mood disorders, anxiety, attention deficit, poor concentration, impaired memory, difficulty in word finding, confusion, visual defects, tinnitus (ringing in ears), vertigo (dizziness), inflammation within the heart (myocarditis or endocarditis), atherosclerosis (build up of plaque within the arteries), shortness of breath, high blood pressure, impaired circulation, Raynaud’s phenomenon (fingers, nose, toes and/or ears become unusually sensitive to cold and may turn white or blue when exposed to cold), Sjцgren’s syndrome (chronic dryness of the eyes, mouth and vagina) and antiphospholipid syndrome (clotting problems, strokes, fetal loss).
Prevention/management: Lupus is difficult to diagnose because of the many different symptoms it can manifest. Generally a person must exhibit 4 of 11 main criteria before a diagnosis can be confirmed. Criteria include: butterfly rash (over bridge of nose and across cheeks), photosensitivity (sensitivity to the sun), discoid rash (disc-shaped rash on face, ears, scalp and torso), mucosal(mouth) ulcers, arthritis, serositis (inflamed lining of the lungs or heart in the form of pleuritis or pericarditis), kidney disorder, neurologic disorder (seizures or psychosis), blood disorders, immune problems and presence of antinuclear antibodies.
Medical treatment consists primarily of nonsteroidal anti-inflammatory drugs (NSAIDs) to manage pain, steroids, antimalarial drugs and immunosuppressant drugs.
Self management therapies include wearing sunscreen, protective clothing and a hat when going outside to protect against photosensitivity, daily exercise to maintain strength, mobility and energy levels, pacing activities and getting adequate rest to help ease fatigue, eating a balanced, healthy diet, avoiding alcohol and ensuring an adequate emotional support system.
Additional information: Lupus Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Foundation, Wikipedia
|
 |
Definition: Macular Degeneration, also known as Age Related Macular Degeneration (AMD), is the loss of the central field of vision from one or both eyes. (The macula, located near the center of the retina, is the area of the eye responsible for high acuity vision.) Macular degeneration does not lead to complete blindness, because people still retain their peripheral vision. However, central vision is required to see objects clearly and therefore to perform tasks such as driving, reading, examining objects in fine detail or recognizing faces.
There are two types of macular degeneration – wet and dry.
- Wet AMD – the most serious type, as it can lead to rapid vision loss if left untreated. With wet AMD, extra blood vessels start growing behind the retina and macula. These blood vessels are fragile and tend to bleed and leak fluid, causing the macula to bulge or lift up, distorting and then destroying central vision. People with wet AMD may see one or more dark spots in the centre of their vision, caused by fluid building up under the macula. Straight lines may appear wavy because the macula is no longer smooth. Some people may have no initial symptoms, but that doesn’t mean the damage is not occurring. About 10-15% of AMD cases are of the wet variety. All cases of wet AMD are classified as advanced AMD because of the seriousness of this version of the disease. Wet AMD is sometimes referred to as neovascular AMD, with neovascular referring to the growth of new blood vessels in an area where they’re not supposed to be.
- Dry AMD – considered less serious because this type of AMD progresses more slowly, but the end result is eventually the same. With dry AMD, cellular debris called drusen accumulate between the retina and the choroid, the thin layer of tissue between the retina and the sclera (white of the eye) which provides oxygen and other nutrients to the retina. Eventually the retina detaches and the macula becomes thin and dried out so that the photoreceptor cells (rods and cones) atrophy due to poor nourishment. The amount of central vision loss (manifests initially as blurry vision and then as blank spots in the field of vision as greater numbers of photoreceptors die) depends on where and by how much the macula dries out. There are 3 stages of dry AMD: early (presence of several small or medium sized drusen with minimal (or no) vision loss), intermediate (more and larger drusen, with some vision loss, particularly in lower light levels) and advanced (a distinct blurred spot in the central vision, which can grow over time). Approximately 85-90% of all AMD cases are of the dry type. However, dry AMD can progress to wet AMD in some, but not all cases. Scientists do not yet know enough about AMD to be able to predict if and when the dry form will turn into the wet form.
There is no known cure for either wet AMD or dry AMD, and in both cases vision loss is irreversible. There is no pain associated with either type.
Macular degeneration is a leading cause of visual impairment in older people, particularly those of Caucasian (white) descent. According to the American Macular Degeneration Foundation, macular degeneration affects more than 10 million Americans. An Eye Disease Prevalence Research Group study reported in the April 2004 issue of Archives of Ophthalmology indicated that macular degeneration is strongly associated with increasing age, particularly after age 60. 1 in 10 white Americans over 80 has vision loss from macular degeneration.
Known or suspected causes: While what specifically causes macular degeneration is not conclusively known, researchers have identified the following risk factors:
- Age: This is generally considered to be the greatest risk factor. According to the Eye Digest published by University of Illinois Eye and Ear Infirmary, approximately 10% of patients 66 to 74 years of age will have findings of macular degeneration. The prevalence increases to 30% in patients 75 to 85 years of age. By comparison, macular degeneration is found in only 2% of middle aged people. According to the Canadian Medical Association Journal (Feb. 17, 2004 edition), significant vision loss from cases of more advanced macular degeneration affects only 1% of people in their 60s but over 15% of people in their 90s.
- Smoking: Smoking appears to be the most significant risk factor in developing macular degeneration next to aging, and it is one of the few modifiable risk factors associated with this disease. In a 2005 review study published on nature.com, 13 out of the 17 studies reviewed showed a statistically significant association between smoking and macular degeneration. One British study found smoking to be associated with approximately 25% of macular degeneration cases with severe vision loss. A 2006 report in the British Journal of Ophthalmology found people living with smokers doubled their risk of developing macular degeneration. The January 2008 issue of Archives of Ophthalmology published a study which evaluated 3,500 residents of Beaver Dam, Wisconsin over a 15 year period and found those who smoked at the initial start of the study had an approximately 45% greater chance of developing early macular degeneration.
It is believed smoking is such a key risk factor because smoking negatively affects a number of processes thought to be involved in the development of macular degeneration, including immune function, depression of antioxidant levels and reduction of choroidal blood flow.
- Family history: The Eye Digest also reports that for people who have a relative with macular degeneration, their lifetime risk of developing late-stage macular degeneration is 50%, which is approximately 4 times higher than for people who have no relatives with macular degeneration.
- Race: Macular degeneration is more common in Caucasians than in African-Americans. One theory is their lighter eye colours contain fewer protective pigments than the darker coloured eyes of non-Caucasians. However, there is conflicting evidence about the theory that extra pigment found in darker eyes protects against eye diseases, including macular degeneration, during sun exposure. A small study reported in the British Journal of Ophthalmology (January 2006) found no connection between the eye disease and sun exposure, and no connection between lighter eye colour and macular degeneration. But a number of earlier studies found a correlation between lighter coloured eyes and macular degeneration.
- Gender: Women appear to be at higher risk for this disease than men.
- Macular degeneration genes: A small number of genes have been shown to be strongly associated with a person’s risk of developing macular degeneration, in that mutations of these genes can trigger the onset of the disease.
- Drusen: While an accumulation of drusen is associated with increased risk of macular degeneration, there are many individuals with large deposits who have normal visual acuity. Therefore, there must be at least one other factor that accounts for the loss of vision.
- Hypertension: In September 2003, Investigative Ophthalmology and Vision Science published the results of a European study which demonstrated that high blood pressure may be associated with development of macular degeneration. High blood pressure damages the blood vessels which supply blood to the eyes and may cause them to leak, which leads to fluid build up in the choroid. This can lead to the more dangerous wet form of macular degeneration.
- Obesity: There is some research to suggest a link between obesity and the progression of early and intermediate cases of macular degeneration to advanced macular degeneration. This link may be related to the physiological changes which occur in an individual as they gain excess weight, including increased oxidative stress, cholesterol and inflammation. These physiological changes lead to decreased levels of lutein and zeaxanthin (antioxidants which protect the eyes from oxidative stress and the high-energy photons of blue light) within the retina. Lipofuscin (fine yellow-brown pigment granules), a by-product of the oxidation of unsaturated fatty acids that is indicative of cell membrane, mitochondria (the part of the cell that generates energy) or lysosome (the part of the cell that disposes of waste by-products) damage, is a major risk factor implicated in macular degeneration.
According to a study reported in Archives of Ophthalmology (June 2003), overweight individuals with macular degeneration had more than double the risk of progressing to more advanced forms of macular degeneration compared to people of normal body weight. On the other hand, compared to inactive patients, those who performed vigorous activity at least three times per week reduced their risk of developing advanced macular degeneration.
- High fat intake: A 2009 study published in Archives of Ophthalmology reported that diets high in saturated and polyunsaturated fats (Omega 6 fatty acids) are associated with an increased risk of macular degeneration, whereas monounsaturated fats appeared to provide a protective effect. It could be that these higher fat diets are poor in many micronutrients that protect against macular degeneration, such as lutein, zeaxanthin and other antioxidants. Diets high in fruits and vegetables, on the other hand, will supply the micronutrients necessary for maintaining good eye health.
- Exposure to blue light: Blue light is high-energy visible light (HEV light) that is part of the visible light spectrum our eyes are able to process, but exposure to this higher frequency can cause radiation damage to the photoreceptors in the eye. Some researchers have therefore theorized that excessive blue light exposure can lead to macular degeneration. This theory has not been proven conclusively, but some research has shown that it may indeed be a contributing factor.
- Drug Side Effects: Some anti-malarial drugs such as Aralen (chloroquine) and anti-psychotic drugs which are phenothiazine based* have been shown to induce macular degeneration. In addition, Fosamax for osteoporosis may predispose one to macular degeneration.
*Thorazine (chlorpromazine), Mellaril (thioridazine), Prolixin (fluphenazine), Trilafon (perphenazine) and Stelazine (trifluoperazine)
- Sleep Apnea: Sleep apnea may be associated with macular degeneration.
Consequences of Macular Degeneration: In the early stages of the dry form of macular degeneration symptoms may not be noticeable, particularly if only one eye is affected because the good eye will compensate for the weak one. However, as the disease progresses to the more advanced stage damage to the macula will become apparent as vision problems begin to manifest. Once macular degeneration has been diagnosed its progress may be slowed, but any damage already done to the eyes is irreversible and the related vision loss is permanent.
Though macular degeneration by itself will not lead to total blindness, one’s central vision may eventually be gone completely, leaving only peripheral vision available. Imagine being able to see only a big black spot in front of you and then just a little bit of the world around you out of the corner of your eye. Try using only your peripheral vision for a little while and you will see how difficult is it to perform simple tasks and visually recognize the people you talk to.
Once central vision loss reaches a critical point, one is classified as legally blind and will no longer be permitted to drive. At this point, one’s independence will be severely compromised and many previously enjoyed activities such as reading, watching TV, participating in group sports, or even taking a simple walk in the park without assistance will no longer be possible to perform.
In the initial stages one may notice blurred or distorted vision (i.e. mini blinds on a window will look wavy instead of straight), making it difficult but not impossible to maintain one’s current lifestyle. The blurriness may disappear in brighter light and those people with early to intermediate macular degeneration may require increasingly brighter light for reading or other close work. They may find it difficult to adapt to low light levels, such as when they enter a dimly lit restaurant. Printed words will become more and more blurry as the disease progresses.
A person may also begin experiencing difficulty in discerning colours, particularly dark colours from other dark colours and light colours from other light colours. Colours (and shapes) may look different when viewed from each eye. Vision may be slower to recover after exposure to bright light and sensitivity to colour contrast may be lost, so that contours (outlines and silhouettes), shadows and colour vision are less vivid.
Objects may start appearing smaller in one eye than in the other (called micropsia), which indicates swelling or bulging of the macula. This bulging increases the distance between the individual photoreceptors in the eye, which makes the object appear smaller to the brain.
As vision loss progresses, vision will become increasingly more hazy so that faces are more difficult to recognize. Scotomas (shadows or missing areas of vision) will appear in one’s field of vision, making it progressively more difficult to function.
Note that the wet form of macular degeneration progresses more quickly than the dry form, so that vision loss may be sudden rather than the gradual process described above.
There is no pain associated with macular degeneration, which is why the disease is often quite advanced before it is diagnosed.
Those individuals diagnosed with macular degeneration can still use their eyes for reading, watching TV and other routine activities. Normal use of the eyes does not cause any further damage to one’s vision.
Prevention/management: Because researchers do not know the exact process which triggers macular degeneration, the best known way to prevent the disease is to reduce or eliminate as many known risk factors as possible from your lifestyle. This would include not smoking, avoiding second hand smoke, watching your weight, keeping your blood pressure under control and exercising regularly.
It would also include eating a healthy diet high in fruits and vegetables to obtain adequate amounts of lutein, zeaxanthin and other antioxidants. According to Wikipedia, the following foods are considered good sources of lutein and zeaxanthin: eggs, spinach, goji berry, kale, turnip greens, collard greens, romaine lettuce, broccoli, zucchini, kiwifruit, corn, garden peas, swiss chard and Brussels sprouts.
In addition, there is evidence to indicate that Omega 3 fatty acids (DHA & EPA) can slow the progression of early stage macular degeneration. They may also be beneficial in slowing the advanced stages when combined with low glycemic index foods. It may therefore be beneficial to incorporate fish, particularly salmon, into one’s diet on a regular basis.
People at risk for macular degeneration may benefit from wearing sunglasses with UV protection whenever they are exposed to the sun.
People diagnosed with early stage dry macular degeneration should have a comprehensive dilated eye exam at least once a year to monitor the progression of the disease. They can also check their vision at home using an Amsler grid, which is a grid of horizontal and vertical lines. Each eye should be checked separately and if any changes in the visual appearance of the grid are detected, a comprehensive dilated eye exam should be obtained.
Once dry macular degeneration reaches the intermediate stage, it can be treated with a specific high-dose formulation of antioxidants and zinc that has been found to slow the progression of intermediate macular degeneration to the advanced stage. Called the AREDS formulation because it is based on the Age-Related Eye Disease Study (AREDS) conducted by the National Eye Institute in 2001, the formulation is much more concentrated than one could obtain from a normal diet. (The National Eye Institute is currently evaluating the protective effects of lutein, zeaxanthin and Omega-3 fatty acids against macular degeneration.)
Though the AREDS formulation is not a cure and will not restore any vision already lost, it may help slow the disease and thus preserve one’s vision for a longer period of time. This is the only available “treatment” for dry macular degeneration at present.
Wet macular degeneration can be treated with laser surgery, photodynamic therapy, and anti-angiongenic injections into the eye, but none of these treatments is a cure - the disease and related loss of vision may continue despite treatment.
Additional information: Wikipedia, American Macular Degeneration Foundation, National Eye Institute, Age Related Macular Degeneration: What You Should Know (National Eye Institute), All About Vision, Eye Center of Northern Florida, Mayo Clinic, eMedicineHealth, Zimbio
|
 |
Definition: According to the National Heart, Lung and Blood Institute (NHLBI), metabolic syndrome (sometimes called sydrome X, insulin resistance syndrome or obesity syndrome) is a name given to a group of risk factors that increase your risk for coronary heart disease and other health problems such as diabetes and stroke. The Institute lists 5 conditions that are known metabolic risk factors for heart disease and states that a person will be diagnosed with metabolic syndrome when they exhibit at least 3 of these 5 symptoms:
- Abdominal obesity, or a large waistline. (Excess abdominal fat is a greater risk factor for heart disease than fat deposits elsewhere on the body.)
- Higher than normal triglyceride levels. (Triglycerides are a type of fat found in the blood.)
- Lower levels than normal of HDL cholesterol. (HDL is the “good” cholesterol because it lowers your changes of heart disease.)
- Higher than normal blood pressure.
- Higher than normal fasting blood sugar. (The level of sugar in your blood after not eating for 12 hours.)
About 47 million adults (approx. 25% of the total adult population) in the US have metabolic syndrome, and with the rising obesity rates these numbers are expected to grow so that in future metabolic syndrome may overtake smoking as the leading risk factor for heart disease.
There are no specific symptoms of metabolic syndrome, except perhaps for the tendency to accumulate excess body fat in the abdominal area. However, some people may exhibit symptoms of high blood sugar if diabetes is also present: increased thirst, excess urination (particularly at night), fatigue and blurred vision. Some people who are also in the early stages of high blood pressure may experience dull headaches, dizzy spells or more nosebleeds than usual.
Known or suspected causes: While the exact cause of metabolic syndrome is unknown, it is closely linked to aging, genetics and lifestyle (being overweight, physically inactive and/or insulin resistant).
According to the NHLBI, Mexican Americans have the highest rate of metabolic syndrome in the US (31.9%), while Caucasians (23.8%) and African Americans (21.6%) are at lower risk. Although there is equal risk between male and female Caucasians, the risk is higher for women in both the Mexican American and African American groups. South Asians have an increased risk for metabolic syndrome, although specific numbers were not provided.
You are also at increased risk for developing metabolic syndrome if either a sibling or parent has diabetes, if you yourself have a personal history of diabetes, or if you are female and have a personal history of polycystic ovarian syndrome (tendency to develop cysts on the ovaries).
People who take certain medications for inflammation, allergies, HIV, depression or other kinds of mental illnesses are at risk because their medication may cause weight gain or changes in blood pressure, cholesterol or blood sugar levels.
Consequences of Metabolic Syndrome: The more risk factors you have, the greater your chance of developing heart disease, diabetes or stroke. NHLBI claims a person with metabolic syndrome is twice as likely to develop heart disease and five times as likely to develop diabetes. MedicineNet.com goes even further, stating that for people with metabolic syndrome, the risk of Type II diabetes is 9-30 times higher over the normal population and the risk of heart disease is 2-4 times higher.
A tendency to form blot clots and/or have low grade inflammation throughout the body are often associated with metabolic syndrome, but the medical community doesn’t know whether these conditions cause or worsen metabolic syndrome.
Approximately 85% of people who have type II diabetes also have metabolic syndrome, and this group is at much higher risk for heart disease than the 15% of people with type II diabetes who do not also have metabolic syndrome.
MedicineNet.com also states that metabolic syndrome can be associated with fat accumulation in the liver, resulting in inflammation and potential for cirrhosis. There is also an association with microalbuminuria, the leaking of protein into the urine, which is a strong indicator of kidney damage. Other problems tied to metabolic syndrome include sleep apnea, polycystic ovary syndrome, increased risk of dementia with aging and cognitive decline in the elderly.
Prevention/management: The best way to prevent metabolic syndrome is with a long term commitment to living a healthy lifestyle.
Treatment focuses first on reducing risk of heart disease and then on preventing type II diabetes if it has not already occurred. Medication can be used to manage metabolic syndrome through treatment of the individual risk factors present – high blood pressure, high triglycerides, low HDL cholesterol, high blood pressure and diabetes. Aspirin may also be prescribed to lower the risk of blood clots.
Additional information: National Heart Lung and Blood Institute, Wikipedia, MedicineNet.com
|
 |
Definition: Multiple Sclerosis, commonly known as MS, is an autoimmune disease which destroys the ability of neurons to properly process and transmit instructions from the brain to the rest of the body. The body’s immune system effectively turns upon itself by destroying the oligodendrocyte brain cells responsible for maintaining the myelin sheath around neurons. As the myelin sheath thins, the quality of the signals between neurons degrades, leading to a variety of problems and symptoms.
In the early stages of MS, as remaining oligodendrocytes try to rebuild the myelin during periods of remission, the oligodendrocytes can't keep up and a scar-like plaque builds up around the axons. The name multiple sclerosis refers to these scars (scleroses) or lesions. Eventually, after the myelin is completely lost, the axons themselves become so damaged they are severed from the main part of the neuron body.
There are four different classifications of MS:
- Relapsing remitting MS (RRMS) – Consists of distinct “episodes”, with extended periods of complete or near-complete remission lasting for several months or even years between episodes. Flare ups can last from a few days to a few months.
- Primary progressive MS (PPMS) – A slow worsening of the disease without any remission periods, although symptoms may stabilize or temporarily improve for a time.
- Secondary progressive MS (SPMS) – Similar to RRMS, but the disease steadily worsens and remissions become less frequent. About 50% of people with RRMS will progress to SPMS within 10 years of diagnosis.
- Progressive relapsing MS (PRMS) – A steady worsening from day one, without remission, with additional attacks where symptoms worsen for a time before settling down. This form of MS is relatively rare, occurring in only about 5% of all cases.
MS most commonly develops in young adults in their twenties or thirties, and in women more often than men in a 3:2 ratio. (Many autoimmune diseases affect women more commonly than men.) It’s estimated there are around 2.5 million cases of MS worldwide. Canada has the highest rates of MS in the world, at 240 cases per 1000 people. (More than 30 cases per 1000 is considered high.) Approximately 3 Canadians are diagnosed with MS on a daily basis.
Known or suspected causes: The exact cause of MS is still unknown. However, there are several theories, including genetics (some specific genes have been linked to MS), infections (i.e. Epstein-Barr virus) and environmental risk factors. It’s also possible MS is caused by a combination of these three variables.
MS has been traditionally classified as an autoimmune disease, but there is growing acceptance that there may be a degenerative aspect to it as well, much like Alzheimer’s disease, cancer, diabetes, heart disease, osteoarthritis, etc. Studies show that plasma homocysteine is elevated in patients with MS, just as it is with other degenerative diseases like coronary heart disease and atherosclerosis. In fact, the level of plasma homocysteine positively correlates with the degree of cognitive and motor impairment found in MS patients. There is also MRI evidence to indicate nerve cell degeneration occurs very early in MS and is not limited solely to MS lesions, giving further credence to a degenerative effect.
While MS is not considered a hereditary disease, the risk of MS is higher in relatives of a person with the disease, particularly for siblings, parents and children. Some reports indicate MS is up to 80 times more common in first degree relatives (i.e. brothers, sisters, or children). An identical twin of someone with MS is 300 times more likely than the general population to develop MS themselves.
MS is more common in some ethnic groups than others, and particularly for those of Northern European ancestry. Although African Americans are less likely to develop MS than Caucasians, when they are afflicted the disease tends to progress more rapidly and they don’t respond well to treatment.
MS is also more common in people who live farther from the equator – decreased sunlight exposure has been linked to higher risk in genetically susceptible people, perhaps because less sunlight leads to less Vitamin D production by the body.
Several studies have shown that smoking is a significant risk factor for developing MS, not only for the smokers, but also for those breathing in second hand smoke, particularly children. The Nurses’s Health Study found the risk of developing MS was 1.6 times greater for women who smoked versus those who didn’t, and risk increased to 1.7 times for individuals who had smoked for 25 years or more. Even past smokers had a 1.2 times greater risk. A Norwegian study provided similar findings in that smokers were 1.8 times more likely to develop MS.
Other environment factors which have been examined but not conclusively proven to cause MS include severe stress, occupational exposures and toxins such as solvents, vaccinations, diet and hormone intake. While major stress events (marriage breakdowns, moving, losing or changing jobs, etc.) has been shown to exacerbate MS episodes, there is no convincing evidence that it causes MS in the first place.
In terms of diet, there is growing evidence to indicate cow’s milk may play a key role in the causation of MS, just as it has been linked to diabetes. (A world wide study is currently underway where children are being kept off cow’s milk to see if it prevents diabetes.) Certain proteins in cow’s milk are very similar to some human proteins, including those which make up part of the myelin sheath. Researchers have theorized that in some cases where the body’s immune system targets cow’s milk protein as a foreign invader, it is then fooled into thinking the similar human protein is also a foreign invader and starts to systematically destroy it.
Italian scientists have recently discovered that people with MS have problems with venous blood (blood circulating in veins, as opposed to arteries) properly draining from the brain, whereas people without MS do not have similar drainage problems. The poor drainage causes disruption to small veins and damages a portion of the brain or spinal cord near the disrupted veins. The scientists suggested the drainage problems could be fixed with minimally invasive surgery and in fact some vascular surgeons are currently doing so with encouraging results. However, the operation is rather controversial at the moment and it will be some time before the jury is in regarding whether the procedure is truly effective or not long term.
Consequences of Multiple Sclerosis: Almost any neurological symptom can occur with MS, including problems with the central nervous system (brain and spinal cord), peripheral nervous system (connects limbs and organs to brain and spinal cord), or autonomic nervous system (heart rate, digestion, respiration rate, salivation, perspiration, diameter of the pupils, etc.). Symptoms experienced will depend on where in the body the nerve signal damage has occurred. For example, motor neuron damage could result in muscle weakness or stiffness, sensory neuron damage might cause tingling, numbness or pain, and optic nerve damage may lead to vision problems. One characteristic symptom of MS is Lhermitte’s sign, which causes an electrical sensation to run down the back when the neck is bent.
Relapses occur more frequency during the spring and summer months. Viral infections like the common cold or influenza can increase risk of relapse. Pregnancy can also increase the risk of relapse, with higher risk being in the first trimester and within the first few months after childbirth.
Symptoms often progress to physical disability, such as changes in sensation (i.e. reduced sense of touch or “pins and needles” feeling), muscle spasms, tremors or weakness, difficulty in moving (including coordination and balance issues), problems with speaking or swallowing, vision problems (involuntary eye movement, inflammation of the optic nerve or double vision), fatigue, acute or chronic pain, and bladder/bowel difficulties. These disabilities can become permanent, even during periods of remission, particularly as the disease progresses.
When neurons inside the brain are affected, varying degrees of cognitive impairment can result. Depression and mood swings are also common.
Even when in remission, neuron damage continues to take place despite a lack of obvious symptoms. 90% of MS scleroses or lesions are below the "clinical threshold" and thus do not produce noticeable symptoms. (In contrast, episodes or relapses indicate an increased level of inflammatory activity in the central, peripheral or autonomic nervous system.) Symptoms may not appear until nerve damage reaches a critical threshold where the body can no longer compensate. When functionality is lost, it will never be regained.
According to the Multiple Sclerosis Society of Canada, as a result of improved treatments people with MS can live a near normal lifespan. However, according to a Danish study completed in 2004, people with MS die an average of 10 years sooner than the general population (particularly if they do nothing to treat their disease), and that approximately 56% die from complications related to MS. Wikipedia notes almost 40% of MS patients will live to at least age 70. The rate at which the disease progresses (and leads to disability) will depend on the type of MS, the individual, and what, if any, course of treatment they choose to follow.
Prevention/management: Because there is no known cure for MS, treatment generally focuses on reducing number of attacks, relieving symptoms and slowing disease progression, thus improving overall quality of life. There are a growing number of drugs available that either reduce inflammation to prevent relapses (immunmodulatory drugs), reduce the severity of symptoms during relapses (steroids), or ease symptoms (different types of medications).
The good news about the evidence pointing to MS being degenerative is that improving one’s overall health through diet and exercise can be of significant benefit to MS patients, just as it is to people with other degenerative diseases such as coronary heart disease and atherosclerosis. In fact, Taking Control of Multiple Sclerosis shows that both a diet low in saturated fat and exercise help maintain fitness and function as well as slow the progression of the disease.
Additional information: Multiple Sclerosis Society of Canada, Taking Control of Multiple Sclerosis, Wikipedia
|
 |
Definition: This is the most common form of arthritis affecting 1 in 10 Canadians and is sometimes referred to as "degenerative joint disease". Estimates regarding the total percentage of population affected vary significantly depending on source consulted, but the National Center for Chronic Disease Prevention and Health Promotion in the US believes osteoarthritis affects 14% of adults aged 25 and older and up to 1/3 of adults over age 65. Women have higher rates than men, particularly in the fingers, and especially after age 50 (i.e. after menopause).
Osteoarthritis slowly destroys the hyaline cartilage (cartilage covering the ends of the bones where they meet to form a joint) of the joints so that the bones start rubbing against each other, leading to chronic pain, swelling and stiffness. Over time the shape and composition of the joint changes so that it no longer functions smoothly, and fragments of bone or cartilage may end up in the joint fluid, causing further irritation and pain. The joint’s ability to absorb shock may be affected.
Symptoms will vary by person, but most common are stiffness, especially upon waking or after periods of inactivity, as well as swelling or tenderness and either steady or intermittent pain in a joint. There may also be a feeling or a sound of bone rubbing on bone when the affected joint is used. Osteoarthritis usually develops slowly, initially starting with an ache after physical work or exercise that progressively worsens over time.
Osteoarthritis is most commonly found in fingers, knees, hips and spine. Other joints which are affected less frequently include wrists, elbows, shoulders and ankles. With the lesser affected joints there is usually a history of injury or unusual stress.
Known or suspected causes: No single, specific cause can be attributed to osteoarthritis, and the current thinking is that cause is related to a combination of genetic and environmental or lifestyle factors. Excess body weight can put significant added pressure on joints, which could cause cartilage to eventually break down over the years. Repetitive movements (i.e. work related repetitive bending, kneeling or squatting) or serious joint injuries may lead to osteoarthritis down the road. Underlying bone or joint disorders or defects could cause cartilage to wear faster so that joints lose their shape and ends of bones begin to rub together.
Established risk factors include:
- Age (the older you are the more likely you are to develop osteoarthritis)
- Gender (more common in women than men, especially after menopause)
- Race (some Asian populations have a lower risk)
- Genetic predisposition (there is some evidence that some types of osteoarthritis may be hereditary – i.e. knees, hips, hands)
- Joint injury or overuse (related to sports, work or trauma)
- Excess body weight (particularly for osteoarthritis of the knee)
- Joint alignment or muscle weakness (a misalignment of the joint can cause excessive wear and tear over time)
Other possible risk factors include:
- Estrogen deficiency
- Osteoporosis (inversely related to osteoarthritis)
- Vitamins C, E and D (conflicting data)
- C-reactive protein (increased risk at higher levels)
Consequences of Osteoarthritis: The joints most commonly affected include the fingers and base of thumb, which is often hereditary. Fingers can become enlarged or gnarled, and small bony knobs may form on either the middle or end joints of fingers. When fingers and thumbs are affected, it is difficult to grasp and/or hold objects or perform delicate tasks such as needlework.
With knee osteoarthritis, stiff, swollen and painful knees make it difficult to walk, climb stairs or get in and out of chairs or bathtubs.
Hip osteoarthritis can lead to pain, stiffness and severe disability. The pain may also be felt in the groin and/or inner thighs. This makes it difficult to move, bend or walk.
Osteoporosis of the spine can lead to stiffness and pain in the neck or lower back, and weakness or numbness in the arms or legs.
All forms of osteoarthritis create stress due to ongoing pain, which tenses the body and makes pain worse. The constant pain and coping with limited or lost abilities can cause significant levels of depression, which makes it even harder to cope with daily living.
Prevention/management: There are no drugs available to treat the specific disease, so the focus is instead on medications which minimize pain and stiffness so that it is easier to remain active and as independent as possible. Physical or occupational therapy may prove helpful, but surgery is usually not necessary, except in cases of severe pain that doesn’t respond to other treatments or there is very limited motion left within a joint.
Glucosamine (plays a role in formation and repair of cartilage) and chondroitin sulfate (contributes to joint elasticity), both found naturally in the body, are two natural dietary supplements which may provide some benefits. A large scale study in the US found these supplements helped those with moderate to severe pain, but had little effect on mild pain.
Other dietary sources of relief may include avocado/soybean oil, boron, boswellia, ginger and SAM-e.
Other treatments for osteoarthritis include: heat (stiff joints) and cold (acute pain) treatments, weight loss (relieves pressure on joints), exercise (range of motion exercises to maintain flexibility, cardiovascular endurance to improve energy and control weight, strengthening exercises to help muscles support and protect the joints), relaxation techniques, massage, electrical stimulation acupuncture, thinking positive and keeping your sense of humour.
While many factors contributing to the development of osteoarthritis are beyond one's control, certain steps can be taken to help minimize the risk of contracting the disease. Protect your joints by avoiding repetitive strain injuries and should an injury occur, ensure it is properly attended to so that it can heal as fully as possible. Ensure you remain at a healthy body weight to protect your knees against excess stress which could over time wear down your joints and allow for osteoporosis to set in.
Additional information: The Arthritis Society of Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Foundation, Wikipedia
|
 |
Definition: Osteoporosis, which means porous bone, is a skeletal (bone) disorder that reduces bone mineral density (quantity) and deteriorates the structure (quality) of bone tissue, resulting in fragile bones and significantly higher risk of fracture. Areas most susceptible to breakage include hip, spine (vertebrae) and wrist, although other bones within the body such as ribs are also at risk.
According to Osteoporosis Canada, 1.4 million Canadians suffer from osteoporosis. It is estimated that one in four women and one in eight men over age 50 have this disease. However, osteoporosis can strike at any age.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases in the US estimates that 50% of women and 25% of men will have an osteoporosis-related fracture in their lifetime.
Known or suspected causes: It is generally accepted there are three main causes of osteoporosis:
- Less than optimal bone growth during childhood and adolescence;
- Increased loss of bone mass, particularly after menopause;
- Bone loss secondary to other diseases and certain medications used to treat them.
Women tend to reach their peak bone mass around age 30 and then level off or decline gradually from there, depending on lifestyle and other health or environmental factors. After menopause (whether naturally or surgically induced through removal of the ovaries), estrogen, which plays a critical role in building and maintaining bones, is reduced to about 10% of pre-menopausal levels. Therefore, immediate bone loss can be quite significant, but this rapid decline tends to level off so that by age 65-70 rate of bone loss is more or less equivalent to that of men. (Men also experience a loss of bone mass as they age (related to a reduction in testosterone), but their rate of decline is more gradual then a woman’s.)
Controllable risk factors for osteoporosis include the following:
- Diet: ensure adequate calcium and vitamin D intake, through supplementation if necessary, and control sodium (excess sodium causes us to excrete too much calcium in our urine) and protein (an adequate level is required to assist in the repair of bone tissue but too much can also cause excessive calcium excretion through urine).
- Smoking: lowers estrogen levels within the body and leads to earlier onset of menopause (which further lowers estrogen levels), plus interferes with absorption of calcium.
- Alcohol: excess intake (as little as 2-3 ounces per day) reduces estrogen production, inhibits the body’s ability to absorb Vitamin D and increases PTH levels which in turn reduce the body’s calcium reserves (PTH increases calcium levels in the blood by removing it from the bones, if required); heavy drinkers are also more prone to bone loss and fractures because of poor nutrition and increased risk of falling.
- Soft drinks: some studies indicate an increased risk, which may be due either to the phosphoric acid in the pop or to soft drinks replacing calcium-containing drinks from the diet.
- Sedentary lifestyle: an inactive lifestyle, whether by choice or due to immobilization through a cast or extended bed rest, does not put enough stress on the bones to keep them healthy; like muscle, bone responds to exercise by becoming stronger.
- Medications: certain medications can contribute to loss of bone density - corticosteroids used for arthritis, asthma, Crohn’s disease, lupus and other diseases of lungs, kidneys and liver, as well as anti-seizure drugs, GnRH drugs used to treat endometriosis, excessive use of aluminum containing antacids, certain cancer treatments and excessive thyroid hormone.
- Estrogen deficiency: whether through early menopause, surgical removal of ovaries or as result of prolonged amenorrhea (abnormal absence of menstruation), hormone replacement therapy is available, but it is not without risks and side effects.
Non-controllable risk factors for osteoporosis include:
- Personal history: if you’ve already had a fracture or have been diagnosed with osteopenia (low bone mass), you are at significantly higher risk.
- Family history: there appears to be a hereditary factor.
- Gender: women have less bone tissue and lose bone faster after menopause.
- Age: bones get thinner with age, so the older you are, the greater your risk.
- Body size: thin, small-boned women are at higher risk.
- Ethnicity: due to lower bone mass and density, Caucasian and Asian women have the highest risk; however, African American and Hispanic women also have significant risk.
Consequences of Osteoporosis: Aside from strengthening our teeth and bones, calcium is required by virtually every cell in the body, including those in the heart, nerves and muscles, to function properly. Therefore, if we do not have enough calcium in our bloodstream, it will be pulled from our bones. Over time this process can significantly weaken bones so that they have an increased risk of fracture in sudden strain, bump or fall situations where normal healthy bones would not break.
There are no symptoms of osteoporosis, so that by the time fracture or deformation occurs the disease is already quite advanced and the individual is at significantly high risk for additional problems. Falls leading to fractures affect one’s mobility, independence, self esteem and overall quality of life. Collapsed vertebrae can produce severe and/or chronic back pain, loss of height and permanent spinal deformities such as a severely stooped posture.
Osteoporosis Canada estimates 70% of hip fractures are osteoporosis related, and that complications (deep venous thrombosis and/or pulmonary embolism) from hip fractures result in death in up to 20% of cases and disability in 50% of those who survive.
Prevention/management: There is no cure for osteoporosis and so the goal of treatment is to prevent fractures.
Note, however, that some bone loss is normal and may not need to be treated unless bones become fragile and prone to fracture.
Various medications exist to build bone density and/or minimize bone loss, but side effects range from nausea and vomiting to bone, muscle or joint aches, sweating, skin rash, eye pain, diarrhea and clot formation, to name a few.
Estrogen or hormone replacement (estrogen + progestin) therapies are also available, but also somewhat controversial. Estrogen therapy has been linked to endometrial cancer (cancer of the lining of the uterus) and at least one major study has linked hormone replacement therapy to a higher risk of breast cancer, heart attack, stroke and blood clots. For these reasons, estrogen and hormone replacement therapies are not recommended long term and non-estrogen medications should be considered first.
The following steps can be taken to help prevent or manage osteoporosis and minimize risk of bone fracture:
- Eat a healthy, balanced diet high in fruits and vegetables and include adequate calcium, vitamin D, and vitamin K.
- Monitor sodium and protein intake to control the amount of calcium excreted through urine.
- Avoid smoking or excessive alcohol consumption.
- Engage in weight bearing exercises (where muscles work against gravity – walking, climbing stairs, dancing, playing tennis) and resistance exercises (weight lifting) to build and maintain bone.
- Develop your balance and flexibility through yoga, tai chi or gentle stretching to reduce risk of falling.
- If you have been officially diagnosed with osteoporosis, avoid spine twisting and bending activities, such as conventional sit ups and toe touches.
- Minimize falls by removing clutter, using nightlights, installing grab bar and rubber mat in bathtub, adding skid-proof backing to carpets and rugs, etc.
- Investigate any changes in vision or hearing that could affect your sense of balance and lead to a fall.
Additional information: Osteoporosis Canada, National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIHSeniorHealth, Wikipedia
|
 |
Definition: Parkinsonism is a general term used to describe neurological symptoms of tremor, hypokinesia (decreased body movement), rigidity, and postural instability, which are caused by lack of dopamine in the basal ganglia area of the brain that controls movement. Parkinson’s Disease is the most common cause of Parkinsonism, but head trauma, some metabolic diseases, exposure to toxins and reaction to medications can also lead to Parkinson-like behaviours.
Parkinson’s Disease is classified as “isolated parkinsonism” in that it is caused solely by a neurodegenerative process without any secondary systemic causes. It belongs to a group of conditions called movement disorders, and is classified as a degenerative disorder of the central nervous system which affects motor skills, speech and other functions. Parkinson’s is both chronic (persists on an ongoing basis) and progressive (symptoms worsen over time). The disease affects everyone differently – some people become severely disabled, while others experience only minor symptoms. At this time it is not possible to predict which symptoms will manifest in a given individual or how intense any of their symptoms might be.
Parkinson-plus diseases, also called atypical parkinsonism, include the classical symptoms of Parkinson’s Disease accompanied by additional symptoms which vary based on type of disease. Approximately 15% of all parkinsonism cases involve Parkinson-plus diseases. Parkinson-plus diseases tend to progress more quickly than Parkinson’s Disease alone, and anti-Parkinson’s medications are generally less effective or sometimes completely ineffective in controlling symptoms.
- Lewy Body Dementia - The most common Parkinson-plus disease, which causes progressive cognitive decline combined with noticeable changes in alertness and attention, visual hallucinations, rigidity and loss of spontaneous movement.
- Multiple system atrophy (MSA) - MSA is the result of degeneration of nerve cells in specific areas of the brain, leading to problems with movement and balance. Other symptoms include lightheadedness or fainting, constipation, lack of bladder control and erectile failure in men.
- Progressive supranuclear palsy (PSP) - Involves gradual deterioration and death of selected areas of the brain, initially causing loss of balance, lunging forward, speed-walking, knocking into objects or people and frequent falling, which then progresses to dementia and slurring of speech, as well as difficulty in both swallowing and moving the eyes.
- Corticobasal degeneration - Includes degeneration of the cerebral cortex and the basal ganglia areas of the brain, leading to disorders of both movement and cognitive function.
According to the Parkinson’s Disease Foundation, as many as one million Americans suffer from Parkinson’s disease, which is more than the total number of individuals afflicted with Multiple Sclerosis, Muscular Dystrophy and Lou Gehrig’s disease combined. While approximately 60,000 Americans are diagnosed with Parkinson’s annually, many cases go undetected because doctors mistakenly assume initial deterioration is part of the natural aging process. Approximately 4 million people worldwide live with Parkinson’s disease.
Parkinson’s disease usually affects people over the age of 60, and men more often than women. While the general population has a 1-2% chance of developing Parkinson’s, the risk increases to 2-4% for those 60 years and older.
Young onset Parkinson’s (before age 40) occurs in 4-10% of cases, depending on which statistics you read. The disease tends to progress more slowly in younger people, although of course everyone is affected differently.
Known or suspected causes: At present time, the true cause of Parkinson’s Disease is unknown. However, scientists have isolated 13 genes affecting dopamine cell function that are associated with Parkinson’s Disease and which can cause the disease in a small number of families.
Even so, only about 5% of all cases in the US are acknowledged as hereditary. Epidemiological studies indicate that first degree relatives (parents, siblings) of people with Parkinson’s have only a slightly higher risk than the general population.
The vast majority of cases are sporadic in that family history and genetics have not been implicated in the onset of the disease. Current thought is that some combination of genetics and environment contributes to the development of Parkinson’s Disease, although these factors may vary from person to person.
However, in some cases a specific cause can be isolated. Toxins, head trauma, anoxia (complete oxygen deprivation) and some drug reactions have all been associated with Parkinson’s disease in certain individuals. Pesticides in particular have been linked to Parkinson’s; studies show that individuals exposed to pesticides had a 70% higher incidence than those not exposed. Individuals living in a rural environment and those who consume well water are also at higher risk, perhaps because their water supply contains traces of pesticides.
Although head trauma is considered by some to a risk factor for Parkinson’s, it could also be that head trauma is a result of early symptoms of clumsiness associated with the disease. Recent studies suggest this may be the case, and that no true relationship between head trauma and Parkinson’s exists.
A synthetic narcotic called MPTP can cause immediate and permanent Parkinsonism if injected, which has allowed scientists to more easily study animals with Parkinson’s symptoms to both learn about the disease behaviour and test treatment options. In addition, it has provided some insight into whether pesticides with similar chemical compositions truly do increase the risk of Parkinson’s.
Consequences of Parkinson's Disease: While Parkinson’s disease is not fatal by itself, those afflicated with it do have a lower life expectancy than the general population, due in large part to complications such as choking, pneumonia and falls that could lead to death. But although the actual disease is not life threatening, its debilitating nature most definitely affects one’s quality of life and independence, particularly for those whose symptoms are severe. For example, simple tasks such as rolling in bed or rising from a seated position can become quite challenging.
As previously noted, some individuals are more afflicted than others. However, this is a chronic, degenerative disease, and so everyone deteriorates over time, albeit at different rates. Progression of symptoms can take up to 20 years for some, but only a few years for others.
Symptoms will vary by individual, depending on where in their nervous system the deterioration is happening. However, there are three key characteristics of the disease which are generally common to all cases: tremor, rigidity and bradykinesia. The combination of tremor and rigidity is what produces the ratchety “cogwheel rigidity” that is visually apparent during voluntary movement. Movements at times can be incomplete, or they may stop suddenly for several seconds.
Greater postural instability and more frequent falls occur as the disease progresses, and in more extreme cases there will be complete loss of physical movement (officially termed akinesia). In addition, patients often develop a shuffling gait which is characterized by short steps and feet barely leaving the ground. Consequently, even small obstacles can cause them to trip and fall. Because neck and trunk are so rigid, multiple small steps are required to make a turn.
In some cases, camptocormia or forward flexion of the spine may occur, resulting in a stooped posture. In severe cases the head and upper shoulders will be bent at a right angle relative to the trunk. Camptocormia, when combined with short, shuffling steps, leads to a progressively faster gait that often ends in a fall.
Scoliosis, or curvature of the spine from side to side, is another possible consequence of Parkinson’s, as is dystonia, which consists of sustained and painful twisting muscle contractions, often affecting the foot and ankle and interfering with gait.
Difficulty in swallowing can lead to drooling or even aspiration pneumonia (caused by foreign objects such as saliva, food or nasal secretion entering the lungs).
Impaired motor dexterity and coordination can make relatively simple tasks such as writing a letter or tying one's shoelaces extremely difficult. Poor motor control over tongue, throat, lips and/or lungs can lead to difficulty chewing, as well as dysarthria (poor articulation of speech caused by neurological problems). Speech can become “monotonic” (soft, hoarse and monotonous) or “festinating” (excessively rapid and poorly intelligible).
Akathisia, or inner restlessness, can make it difficult to sit still or remain motionless.
Neuropsychiatric disturbances, which include cognition, mood and behavior problems, can be as disabling as motor symptoms. Mild cognitive “disturbances” occur even in the initial stages, and a large percentage of sufferers will progress to cognitive “impairment” as the disease progresses. This can include slowed cognitive speed, memory problems and poor attention span, as well as other difficulties. As many as 80% of cases will eventually result in full scale dementia. Dementia not only reduces quality of life for both sufferers and caregivers, it increases both risk of mortality and the odds the patient will end up in a nursing home.
Behaviour and mood alternations generally occur, regardless of whether cognitive problems or dementia is present. Depression, apathy and anxiety are quite common. Certain medications used to control symptoms can cause obsessive-compulsive behaviours such as cravings, binge eating, hypersexuality, and pathological gambling.
Sleep problems, excessive fatigue and chronic pain are all fairly common symptoms of Parkinson’s disease. Other potential symptoms include excessive sweating, urinary incontinence, constipation, reduced sense of smell, paresthesias (pins and needles sensation), vision abnormalities, oily skin and orthostatic hypotension (dizziness when standing up due to sudden change in blood pressure).
Prevention/management: Because there are no definitive blood or other laboratory tests to conclusively identify Parkinson’s, diagnosis of the disease can be problematic. Doctors must rely on medical history and neurological examination through interview and observation, using the Unified Parkinson’s Disease Rating Scale as a guide. Doctors will typically look for classic symptoms like shuffling feet and lack of swing in the arms, stiffness in limbs and neck, tremor in the limbs, poor balance and whether or not expression is animated. Brain scans and other lab tests can be used to rule out other diseases, but CT and MRI brain scans of people with Parkinson’s disease usually appear normal.
Because there is no known cure for Parkinson’s disease, disease management focuses on maximizing quality of life as long as possible through the following methods:
- Medication or surgery to control symptoms.
- Physical therapy to help with mobility, flexibility, balance, fatigue and weakness.
- Occupational therapy to help with daily activities.
- Speech therapy to help with voice control and swallowing issues.
- Exercise programs to help muscles and joints and improve overall health and well being.
- Nutritional counseling to help with constipation and gastroparesis (delayed stomach emptying), and to generally support overall health.
- Support group services to help patients and family members more effectively cope with the traumatic effects of this debilitating disease.
There are various medications that may be used alone or in combination to control symptoms. However, many of these medications lose their efficacy as time progresses and/or have undesirable side effects. Type and/or dosage may therefore have to change periodically. Scientists are presently researching some drugs that may slow disease progression by protecting neurons from cell death, but these drugs are still under evaluation.
In advanced cases where medication is no longer sufficient or effective, surgery in the form of deep brain stimulation is an option. Deep brain stimulation was developed in the 1990s and is now a standard treatment worldwide. Electrodes are inserted into the affected areas of the brain and an impulse generator similar to a pacemaker is implanted under the collarbone to provide an electrical impulse to a part of the brain involved in motor function. While this surgery neither cures nor slows disease progression, it can help relieve symptoms and improve quality of life for five years or more. (Like any other surgery, there are risks and some individuals have experienced loss of cognitive function.) While deep brain stimulation is presently the most common surgical treatment, other promising options are being explored, including stem cell development into brain neurons and their transplantation into the brain.
Physical therapy includes both exercises performed in a rehabilitation facility and those that can be done at home. There is some speculation that exercise might stop the progression of Parkinson’s because it produces a neuroprotective mechanism. Regardless of whether that’s the case, exercise will certainly help with balance, joint function, rigidity relief, cardiovascular fitness, muscle strength and flexibilty. It will also help build confidence and reduce stress as patients find they are better able to perform daily activities.
A balanced diet will help improve digestion and thus alleviate the common symptoms of constipation and gastroparesis. High fibre foods such as whole grain breads and cereals, fruits, vegetables and plenty of water are recommended, while caffeine, alcohol, salts and excessive protein should be avoided. Supportive nutrients such as L-tyrosine (an amino acid), ferrous iron and certain coenzymes ("helper molecules" that assist in chemical reactions) have been shown to relieve symptoms to varying degrees. Vitamins C, E and coenzyme Q10 are thought to lessen cell damage due to their protective antioxidant effects, although no conclusive evidence for this protective effect exists. Other compounds which show promise but still require further testing are creatine (increases levels of phosphocreatine, which is an energy source in muscles and the brain) and glutathione (an antioxidant that may protect against nerve cell damage).
Additional information: Parkinson’s Disease Foundation Parkinson Society Canada National Institute of Neurological Disorders and Stroke Medline Plus Wikipedia
|
 |
Definition: A narrowing of the blood vessels outside the heart and brain (i.e. those carrying blood to the legs, arms, stomach and kidneys) due to fatty deposits (plaque) building up in the inner linings of the artery walls. This is very similar to coronary artery disease, except that coronary artery disease involves the blood vessels supplying blood directly to the heart.
Known or suspected causes: People who smoke and/or have diabetes are at particularly high risk. Smokers may have up to 4 times the risk. Other risk factors include a family history of PAD, obesity, physical inactivity, high blood cholesterol, high blood pressure.
Consequences of Peripheral Artery Disease: A common symptom of the early stages of this disease is cramping of the hips, thighs or calves during activity such as walking, climbing stairs or exercising, which subsides a few minutes after activity ceases. However, many people have no symptoms at all.
It is possible to mistake leg pain associated with PAD as part of the normal aging process. However, keep in mind that pain or stiffness as we age occurs in the joints, whereas pain from PAD occurs in the muscles.
As the disease progresses, symptoms progress to leg pain that doesn’t go away once activity ceases, foot or toe wounds that won’t heal or do so very slowly, gangrene and/or a noticeable decrease in the temperature of the lower leg or foot compared to the rest of the body.
More serious consequences include possible loss of a leg. There is also increased risk of heart attack or stroke because people with PAD could have coronary artery disease as well.
Prevention/management: Most people can be treated with a combination of medications and lifestyle changes, which include quitting smoking, controlling diabetes and blood pressure, increasing physical activity and eating a low saturated fat/low cholesterol diet.
When lifestyle changes alone aren’t enough, angioplasty or surgery may be required. Angioplasty involves inserting a thin tube with a deflated balloon on the end into the artery to the area where the build up of plaque is situated. The balloon is then expanded to compress the plaque against the artery so that blood may flow more easily. Sometimes a “stent”, a cylindrical wire mesh tube, is placed there to keep the artery open. When the plaque build up involves a lengthy segment of the artery, surgery is undertaken to attach a vein from another part of the body (or a synthetic blood vessel) above and below the affected area in order to bypass the blocked section of the artery.
Additional information: Heart and Stroke Foundation of Canada, American Heart Assocation
|
 |
Definition: An autoimmune disorder which produces chronic inflammation of the joints when the body’s immune system mistakenly attacks the synovium, or thin membrane lining the joints.
This results in joint damage, ongoing pain, tenderness, stiffness, swelling or inflammation, warmth and redness, loss of function and disability. Joints may also lose their shape, resulting in loss of normal movement. The joints most commonly affected are those of the hands, feet, wrists, elbows, knees and ankles, although the neck, shoulders and hips can be affected as well. Rheumatoid arthritis usually affects both sides of the body evenly, so that if one elbow is affected, then so is the other. The disease can affect many organs, including the skin, heart, blood vessels and lungs.
Other symptoms include fatigue and occasional fever. Tear glands and salivary glands can also become inflamed. Though chronic, symptoms can come and go so that periods of mild activity or perhaps even remission can be punctuated by flare ups.
As the disease progresses, about 20-30% of people develop rheumatoid nodules, small lumps of tissue under the skin of the elbow, hands, back of the scalp, over the knee or on the feet or heels. These nodules usually aren’t painful.
Known or suspected causes: According to Arthritis.com, this disease affects 1% of the adult population in the US and generally affects people between ages 20 and 50. Rheumatoid arthritis is typically 2-3 times higher in women than men and while incidences of the disease for both sexes peak in their sixties there is some evidence that the world wide incidence of rheumatoid arthritis is decreasing. According to the Arthritis Foundation, 70% of those affected by the disease are women.
Despite intensive research, the exact cause of rheumatoid arthritis remains unknown, but it is generally agreed that a combination of genetic and environmental factors are at work. Because RA is not caused by a single gene, it’s not likely children will inherit the disease from their parents, but risk will be slightly greater.
No definite risk factors have been identified to date, but possible factors include sex (women are two to three times as likely as men to develop rheumatoid arthritis), hormonal exposures, tobacco use, dietary components, genetic factors, infection and exposures to bacteria or viruses. There is some indication that rheumatoid arthritis may also be triggered in response to stressful events such as physical or emotional trauma.
Women who have used oral contraceptives may have a slightly reduced risk of rheumatoid arthritis. Recent studies have found rheumatoid arthritis is less common among women who breastfeed and that women who have never had a live birth have a slight to moderate increased risk.
Consequences of Rheumatoid Arthritis: Those with rheumatoid arthritis are at higher risk for other autoimmune diseases such as type 1 diabetes and autoimmune thyroiditis. They also experience a higher rate of infections, lung disease, kidney disease, cardiovascular disease and gastrointestinal problems. Keeping rheumatoid arthritis under control can help reduce the risk of developing these serious health problems.
Prevention/management: No specific test for rheumatoid arthritis exists; instead a number of specific criteria must be met before a diagnosis of the disease can be made. These criteria are based on clinical observation, laboratory tests (including blood tests to see if antibodies to rheumatoid factor (RF) or cyclic citrullinated proteins (anti-CCP) exist) and x-ray evidence of joint erosion.
There is no cure for rheumatoid arthritis and irreparable damage can occur quite early in the disease process, so early aggressive treatment is recommended to alleviate symptoms and slow the progression of the disease. Should damage to joints lead to significant deformity and disability, joint replacement surgery may be warranted.
Medications used in the treatment of this disease include nonsteroidal anti-inflammatory drugs (NSAIDs) for pain, corticosteroids to control inflammation, DMARDs (disease modifying antirheumatic drugs) to slow or modify the course of the disease and biologic agents to block specific steps in the inflammation process without wiping out the entire immune system.
In addition to medication, exercise is important to help ease pain and increase joint mobility. Eating a healthy diet (low in saturated fats and high in unsaturated fats, especially fish oils) and maintaining a healthy weight, along with avoiding smoking and consuming excess alcohol are also recommended.
Research has shown that omega-3 fatty acids taken in large quantities modify inflammation associated with rheumatoid arthritis and that oil extracted from the borage plant has similar properties to NSAIDs without the gastrointestinal side effects. However, effective dosages and long-term side effects of these supplements are not yet known.
Because the exact cause of rheumatoid arthritis has yet to be determined, no specific steps to prevent the onset of this disease can be identified at this time.
Additional information: The Arthritis Society of Canada, National Center for Chronic Disease Prevention and Health Promotion, Arthritis Today, Arthritis Foundation, Arthritis.com, Wikipedia
|
 |
Definition: Pauses in breathing during sleep longer than 10 seconds where there is either neurological arousal (as measured by a shift in EEG readings) and/or a drop of oxygen levels within the blood of 3-4% or more. 5 or more such episodes within a one hour period is considered clinically significant.
There are three types of sleep apnea. The most common form is obstructive sleep apnea, where there is a blockage of the airway usually caused by the soft tissue in the rear of the throat collapsing and closing during sleep. Central sleep apnea is where the brain fails to send a signal to the muscles to breath. Complex sleep apnea is a combination of obstructive and central sleep apnea.
According to Wikipedia, 84% of sleep apnea cases are of the obstructive type and then complex sleep apnea accounts for the vast majority (15%) of the remaining cases. Central sleep apnea by itself accounts for only .4% of all cases.
Known or suspected causes: Obstructive sleep apnea: low muscle tone and soft tissue around the airway (i.e. due to obesity) and structural features that create a more narrow airway. Central sleep apnea: central respiratory depressants such as alcohol, opiates, barbiturates, benzodiazepines and other tranquilizers. Premature babies with immature brains and reflex systems are also at risk for central sleep apnea, but most grow out of this as they mature. Some theorize that sudden infant death syndrome may be related to central sleep apnea.
According to the American Sleep Apnea Association, sleep apnea is as common as adult diabetes, affecting more than twelve million Americans. Risk factors include being male, overweight, and over the age of forty, but sleep apnea can strike anyone at any age, even children. Most sufferers snore, but not everyone who snores has sleep apnea.
Consequences of Sleep Apnea: Most individuals with sleep apnea are not aware they have it so the disorder can go undiagnosed for years. Because during each episode of sleep apnea the brain will eventually rouse the body to start breathing again, sleep patterns are disturbed enough that daytime fatigue is a common symptom. Chronic fatigue can affect one’s ability to concentrate, leading to job impairment or even more disastrous consequences such as motor vehicle crashes.
Additional consequences include memory problems, weight gain, impotency, headaches, high blood pressure and other cardiovascular disease which could result in a stroke or heart attack. (Wikipedia reports that individuals with obstructive sleep apnea have a 30% higher chance of heart attack or other premature death than those without the sleep apnea disorder.) The most serious complication is a severe form of congestive heart failure called cor pulmonale.
Prevention/management: Keep your weight under control so that excess fat does not build up around the neck area and narrow your airways. Avoid alcohol and other central nervous system depressants such as pain killers, sedatives, and muscle relaxants, or at least do not take them around bed time.
Obstructive sleep apnea can be managed in several ways. Sleeping on one side or in an inclined position as opposed to flat on the back helps reduce the risk of the tongue falling back over the airway and/or the airway muscles and other tissue (like the tonsils) collapsing and blocking the airway. There are “oral” or “dental” appliances on the market that push the lower jaw forward and/or prevent the tongue from falling back over the airway. Continuous positive airway pressure (CPAP) machines keep the airways open through a flow of pressurized air into the throat and in more severe cases a NIPPY machine assists with both inhaling and exhaling.
In more severe cases, surgery to anatomically alter the airway is available, including the nasal passage, throat (pharynx), base of tongue and facial skeleton.
Additional information: Canadian Lung Association, Wikipedia, American Sleep Apnea Association
|
 |
Definition: An inflammatory bowel disease (IBD) causing chronic inflammation (swelling) of the inner mucosal lining (first layer) of the large intestine (colon). Ulcerative colitis generally begins at the lower end of the colon just above the anus and extends upwards as the disease progresses. The degree of progression varies by individual, depending on the severity of the disease, and can advance all the way up to where the colon joins the small intestine. The inflammation is believed to result from a malfunction of the immune system whereby white blood cells attack and ultimately damage the lining of the colon, creating ulcers or open sores that bleed and produce pus as cells lining the colon die.
Some individuals go into remission after an initial attack and perhaps have intermittent flare ups, while others are chronically affected with ongoing, continuous disease. About half of all sufferers experience mild symptoms while the remainder are more severely affected.
Ulcerative colitis differs from Crohn’s disease, which involves all layers of the intestine and can affect both the large and small intestines. However, many of the symptoms are similar and so it is sometimes difficult to correctly diagnose which disease is present.
Note that ulcerative colitis is unrelated to ulcers which occur elsewhere in the gastrointestinal tract, such as stomach or duodenal ulcers.
Known or suspected causes: While the exact case of ulcerative colitis is unknown, researchers have been evaluating many potential causes, such as infection, stress, allergies and toxins. Current thinking is that something triggers the body’s immune system to turn on its own bowel. However, since the surgical removal of affected tissue appears to cure the disease, this suggests to some that the problem is with the colon as opposed to the immune system.
The incidence of ulcerative colitis appears to be greater in northern countries such as Canada, northern US, UK and Scandinavia. The disease generally manifests between the ages of 15 and 25 and affects women more than men. Jewish people appear to be the highest risk group.
Genetics are also thought to play a role, since up to 20% of people with ulcerative colitis have a family member or relative with either colitis or Crohn’s disease.
Consequences of Ulcerative Colitis: The most common symptom of ulcerative colitis is blood in the stool, which occurs in over 90% of patients. Diarrhea occurs in about 80% of patients, and may be accompanied by mild to severe crampy abdominal pain. Sufferers can have anywhere from 3 to 20 bowel movements daily, and in severe cases sometimes even during sleep.
If diarrhea and blood loss is excessive, fever and/or weight loss may occur. Hospitalization may be required in those extreme cases where severe bleeding or diarrhea causes dehydration. A special diet, feeding through a vein or sometimes even surgery may then be warranted.
In some cases, ulcerative colitis may trigger inflammation outside the intestinal tract, such as in the eyes or joints, and can also trigger ulcers in the mouth, arthritis, skin lesions, liver disease, inflammation of the bile ducts, osteoporosis and deformation of the fingers (clubbing). The cause of these conditions is not known.
Other symptoms can include anemia that may require iron supplements or blood transfusions, incontinence (loss of bowel control), fatigue, loss of appetite, rectal bleeding, loss of body fluids and nutrients and growth failure in children. In rare cases the colon can swell so much toxic megacolon develops where patients are extremely ill and could require surgery to prevent colon rupture if they don’t respond immediately to medication.
There is an increased risk of colorectal cancer over the long term (i.e. 8-10 years with the disease present), depending on the progression of the disease (i.e. how much of the colon is affected). However, ulcerative colitis generally affects quality of life as opposed to life span.
Ulcerative colitis can usually be cured by surgical removal of the large intestine, but this is generally avoided except in the more severe cases.
Prevention/management: Treatment depends on the severity of the disease and falls into two main categories – treatment of the symptoms and treatment of the inflammation. Treating the symptoms does not affect the basic disease, but it does help patients feel better.
There are several ways to manage inflammation. Adequate rest is critical to healing, so diet must be easy to digest and free of irritants or stimulants. Proper nutrition is also important to healing, so dietary supplements, special elemental (predigested) diets and occasional intravenous nutrition may be required. Medications (anti-inflammatories, corticosteroids, immunomodulators) to induce remission and then prevent relapse are also available and many are safe for long term use.
For those who do not respond to medication or are at risk for colon cancer (i.e. either abnormal or cancerous cells are detected), surgery to remove a portion or perhaps the entire colon may be warranted. 25-40% of ulcerative colitis patients must eventually have their colon removed if medication fails or if side effects of drugs being taken are adversely affecting the patient’s health. In many cases the small intestine can be used to create an internal waste pouch (ileoanal anastomosis) so that normal bowel movements may still pass through the anus. Otherwise, an ileostomy which brings the small intestine to the surface of the skin so that an external waste pouch can be connected will be required.
Additional information: Canadian Society of Intestinal Research, HealthyOntario.com, Wikipedia, National Digestive Diseases Clearinghouse, Medicine Net
|
The information contained in this site is for educational purposes only and should not be used as a substitute for personal care by a licensed physician.
Please see your physician for diagnosis and treatment of any concerning symptoms or medical conditions.
Coming Soon: |
Dementia |
Heart Attack / Stroke |
Muscular Dystrophy |
Allergies |
Bipolar Disorder |
Anemia |
Depression |
Glaucoma |
Alzheimers Disease |
Anorexia / Bulimia |
Obesity |
AIDS |
Hepatitis |
Obsessive Compulsive Disorder |
Thyroid Disease |
Migranes |
Pancreatitis |
Aneurysm |
TOP
© Copyright 2008-2015, Positive Impressions®. All rights reserved. |
|